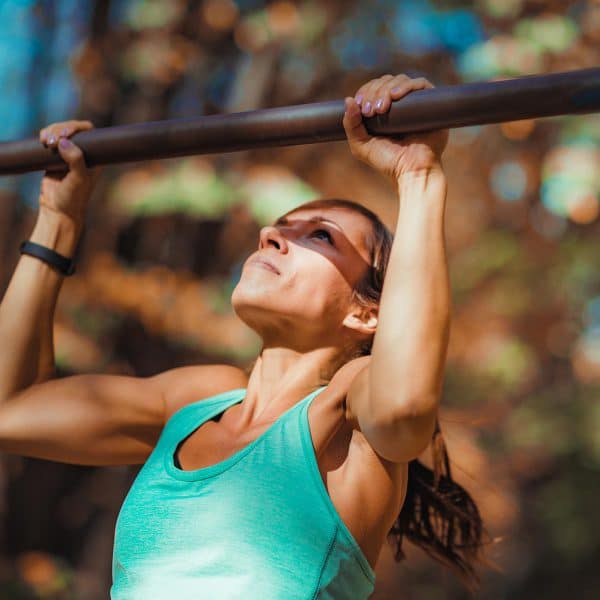
Incontinence, prolapse, anal leakage or pelvic pain? Your pelvic floor supports you through everything in life however including keeping key organs in place. Many of the complaints with aging go back to pelvic floor health, so why is there not an emphasis on it’s care? Kim Vopni is the founder of Pelvienne Wellness Inc – a company offering pelvic health programs and coaching for women in pregnancy, motherhood and menopause. In women’s health circles online, Kim is known as The Vagina Coach. She is a certified fitness professional, creator of the Buff Muff Method and Membership, author of the book Your Pelvic Floor, and a women’s health educator who co-hosts of the Pelvic Love Retreat. In this episode of The Health Fix Podcast, Dr. Jannine Krause interviews Kim Vopni about pelvic health from preparing for childbirth to lowering the chances or reoccurrences of pelvic surgery and why pelvic floor health is necessary to age well.
Dr. Krause’s Protocols
Instructions Included
Traveling soon? Looking to detox or reset your gut? Try one of Dr. Krause’s Fullscript plans.


What You’ll Learn In This Episode:
- You can prep your tissue and pelvic floor for childbirth
- The importance of seeing a pelvic floor therapist annually
- Why Kegels aren’t working for you
- How constipation and dehydration worsen your bladder leakage
- Why there’s a high recurrence of issues post pelvic surgery like prolapse and rectocele
- The two concepts to master to improve your pelvic floor health
- How pulling pelvic floor muscles off the bone during childbirth causes pelvic floor issues
- Lowering of UTIs with estrogen support vaginally
Resources From The Show:
- Kim’s Website – Vagina Coach
- Buff Muff Method $17 and 28 day challenge
- Training the pelvic floor in fitness certificates
- Epi-No – preparing women for child birth – available in Europe.
- Bellies Inc – available in Europe
- Dr. Shobeiri, Urogynecologist in DC – specialist in Levator Ani – avulsions
Our Partners



Podcast Transcript
2:16 – Kim’s backstory
13:20 – Postpartum pelvic floor care
17:36 – What does a Postpartum pelvic floor program consist of
23:47 – What moves the needle the most for prolapse and incontinence
25:11 – The Buff Muff Challenge
30:32 – What impact do meshes. lifts, and slings have on the pelvic floor
35:08 – Prolapse
41:43 – Levator avulsion
46:46 – Could a ski injury cause a levator avulsion
51:02 – GSM or vaginal atrophy
58:57 – Teaching about the pelvic floor in fitness education
102:11 – Where to find Kim online
[Intro] Welcome to The Health Fix Podcast, where health junkies get their weekly
fix of tips, tools, and techniques to have limitless energy, sharp minds, and fit
physiques for life.
Hey health junkies, on this episode of The Health Fix Podcast, I’m interviewing
Kim Vopni. She is the founder of Pelvian Wellness, a company offering pelvic
health programs and coaching for women in pregnancy, motherhood, and menopause.
Now, in online circles and women’s health groups, Kim is known as the vagina coach and she is a
spitfire full of information. Kim is a certified fitness professional, a published author and a
women’s health educator. She’s the creator of the Buff Muff Method and Membership. She’s the author
of Your Pelvic Floor and one of the hosts of The Pelvic Love Retreat. Today, Kim and I are going
to be talking about pelvic health as not only something to do and get pelvic health PT per se
as a means to fix a problem but as a lifestyle keeping your pelvic floor healthy for life and
Kim wants everyone to know that it is never too late to start working on your pelvic health. I
learn a ton in this podcast from how to prevent tearing during childbirth to lowering the chances
or reoccurrence of pelvic surgery. Ladies, this is one podcast you do not want to miss and you will
want to share with your friends and family. So let’s introduce you to Kim Vopney.
JANNINE: Kim, welcome to the
Health Fix Podcast.
KIM: Thank you for having me. Happy to be here. Oh my gosh, it’s been a long time
coming since we have a mutual friend, Dr. Brianne Grogan, and I’ve watched you guys work together on
different things. And I was like, I need to talk to this gal. I need to have her on. And really what
sparked some of this was I started to have some issues with incontinence while I’m doing my workouts,
different jumps, different squats, different things started causing trouble. And I was like,
okay, I need to reach out. And then I saw that you had and app and all these beautiful things.
So tell us a little bit just so my folks can kind of get a little background on you. What
What brought you to specialize in pelvic and vaginal health?
KIM: I know it’s not something you think of growing up aspiring to be right.
I remember wanting to be a dolphin trainer.
That was a fun life goal I had.
So long story was long story made short.
I saw a childbirth video in sex ed class and I said,
I don’t want anything to do with that, but it did spark a bit of a curiosity.
And I started to ask my mom questions and look at the women in my life a little bit
differently and thought, well, they all got all done and they’re carrying on.
So I sort of grew up with this fear fascination of birth and I really was pretty adamant that I
wasn’t going to have children. Then when I did decide I wanted to start a family,
I was determined to have a different story than my mom who I did witness having surgery for
incontinence, having chronic back pain, having a tummy that wouldn’t flatten, avoiding certain
exercise and activities, having hysterectomy. Like I was witnessing all of this and I was really
determined to have a different story. So I thought, okay, well, I’ll just have a cesarean section and
and that will solve all my problems,
and my pelvic floor will be fine.
And through that process of learning more about that,
I realized it’s not the magic.
Just take cesarean and everything’s gonna be fine.
Or you could arguably have some increased risk
for some things.
So my midwives had recommended a product to me
called the Epi-No.
Epi-No stands for No Epizotomy,
and it’s a product made in Germany.
A physician from Germany was in Africa
and witnessed women using gourds of increasing size
to prepare their perineum and pelvic floor for birth.
And he thought, well, that’s a great idea,
but that’s not gonna fly in North America.
So let’s see if we can make something a bit more mainstream.
So he worked with doctors, midwives, physiotherapists
and designed a medical device.
And my midwives told me about this.
I purchased one used to have a great experience
and I thought, why doesn’t everybody have one of these?
So I contacted the company and said,
could I be a distributor here in Canada?
And I didn’t intend for it to be a business.
I thought I’ll just sell a few on the side.
And I did at the start, it was just sort of a little side gig.
And then I was laid off in 2009 from my corporate job.
I was working in human resources.
And I had previous, my previous life,
I had been in fitness, I was a personal trainer.
And as I started now promoting this product
and trying to make it more of a business,
all the principles I was talking about
were fitness focused stretch and strength
and preparation for a physical event.
and how are we going to recover more optimally.
And so I started to meet Commerce Store,
added pelvic health products,
then I started to see, well, okay, now I’m wanting women
to know this information ahead of an event
that is very common in female bodies
that is a major contributor to pelvic floor dysfunction.
So I created a program called Prepare to Push
and it was meant to help educate women
about the pelvic floor prior to birth,
how they could prepare for birth,
how they could use movement,
how they could recover.
And ultimately, of course, I was wanting them
to buy an epi-note as well.
Then I recognized the post-partum recovery period
was so overlooked.
So I ended up forming a second business
with two other women called Belli Zink.
And we wanted to take inspiration from other cultures
around the world who use belly wrapping
and really honor that post-partum recovery phase of life
that we hear as soon as you’re pregnant,
or sorry, as soon as you’ve given birth,
you can’t look pregnant.
You have to erase all signs.
It becomes a place of shame, this belly that you have,
and you’re back at the gym two weeks,
postpartum and everybody’s giving you high fives.
So we wanted to change that
and bring old traditional practices
into the more modern day realm
and incorporate pelvic floor exercise and recovery.
So we did that and was juggling the two for a while,
created a certification course for other fitness
and health professionals within our scope
of not being internal therapists.
How could we help spread the word?
And so that’s been a 19 year journey now,
all that this little side thing that I started,
it’s morphed and evolved in a lot of ways.
But ultimately, I’m very passionate
about increasing awareness and education
around pelvic health and incorporating fitness
and movement and lifestyle principles
to the pelvic floor rather than thinking of it
just being just your kegels
and everything’s gonna be solved.
It’s a much bigger conversation than that.
And so that’s how it all happened.
JANNINE: I am fascinated by this epinec thing.
Like, are you still selling these?
I didn’t see that.
I wasn’t diving very deep.
And that’s apartment on your website.
Are you still selling those?
KIM: No, so what happened with that is
I was the Canadian importer distributor for 14 years.
And then Health Canada, which is like the FDA,
they implemented a new medical device regulation procedure.
or process plan, whatever you want to call it, that had a lot more hoops to jump through,
it was a lot more costly for companies.
And the manufacturer in Germany, Texana, as the name of the manufacturer, they sort of
said, “You know what?
We’re not prepared to jump through all these hoops.
We’ve been here for 14 years.
We know the products, we’ve gone through all of these safety standards already.
This is just a make money scenario for the government.”
they chose to leave Canada.
And I fought so hard, I fought, but I was written up
in the Globe and Mail, which is a major newspaper about this,
because it wasn’t just them.
It was hundreds of smaller companies
were choosing to leave Canada because of it,
because of the additional layers and additional costs.
And it was so sad, because so many incredible products now
weren’t available for people anymore.
So that was at the end of 2018.
And so with that, I closed down my e-commerce store
because it was the main part of my e-commerce.
And I wasn’t prepared to keep all of that other stuff
with I didn’t have that main one.
And then Belly Zinc, which we did have a physical product
that we manufactured as well,
I ended up selling that, the product side of that business
as well.
And that was sort of the, thankfully, transition
to being totally online before the pandemic hit.
And yeah, so Belly Zinc still exists.
The epi-no still exists.
It’s just not available in North America, unfortunately.
JANNINE: Ah, so ladies, if you’re planning on getting pregnant
and wanting to work on things, go to Europe and grab one.
‘Cause I mean, I don’t think I’ve ever heard of,
I’m thinking through like my training, right?
And thinking through of the nurse midwives, I know,
I’ve not heard of anything to prep the tissue
and prep the pelvic floor or child care.
KIM: Yeah. I know when you learn about the product and the philosophy behind it,
it makes so much sense. And then, you know, again, from a fitness and movement perspective,
that’s how we train. That’s how we prepare for physical events, sprints, mountain climbs,
races, whatever we’re doing. We do the principal specificity. We have a training protocol. We follow,
we have a built-in recovery practice. And this product, the epi-no, incorporates all of that
same philosophy using biofeedback. So it helps women see and feel and connect with a part of the
body that we can’t physically, like we can’t see our pelvic floor muscles, they are inside.
So we see our external genitalia, but we don’t, we’re, and many people are often very disconnected
from that part of the body. So using biofeedback, which the epi-no is not the only biofeedback
device, it was the only one really for birth prep, but many physiotherapists will use probes and
and other types of biofeedback to help women connect with that group of muscles.
But if we understand the greatly increased risks of pregnancy and childbirth to the pelvic
floor into optimal function, why we are not doing more ahead of time to educate and step
in with, you know, some people view it as an intervention, but I’m all for an intervention
that’s going to help prepare the body and the person for this upcoming event and also
in part the importance of this group of muscles that nobody really seems to pay attention to
until there actually is a problem.
JANNINE: You’re so on point on that.
I mean, even as a doc, right?
I didn’t specialize in this department.
I actually don’t have children to this day thinking probably I was watching that same
video you were watching and you took it upon yourself to do something about it.
I just went, nope, disconnect, not going to do that.
You know, I don’t know.
But what you’re describing to me, you know, let’s put it this way.
I’ve run a lot, I’ve been in a lot of mountain bike races
and marathons.
I wouldn’t just do it out of nowhere.
KIM: Exactly.
JANNINE: Most women childbirth is longer
than I’ve spent running a marathon,
even my slowest ones.
And like, it’s like a light bulb in my head right now
going like, oh my goodness, you know.
KIM: Well, and you hear, so often you hear kind of
anecdotally, oh, birth is like running a marathon.
No, it’s like four, five, six, even more marathons.
And what happens, as you say, you prepare for that marathon.
You don’t just decide to run a marathon and go and run for four hours.
You have a training protocol and you have nourishment and you have recovery.
And there’s so many elements built in and then pregnancy and child birth is just like,
well, they’ve been doing it for centuries, so I guess I’ll be fine.
And we just sort of, we have this go with the flow mentality that really just isn’t serving us.
JANNINE: It isn’t, it isn’t and it makes sense to prep for this.
So, okay, ladies who are listening,
I know you let a lot of people who listen to my podcast are older, but hey, let’s face
it, a lot of us tend to get pregnant a lot later in life now.
And at that point, I’m thinking, gosh, you know, we could benefit from this.
You can tell your kids, grandkids, tell everybody, tell everybody.
KIM: And you can take the same philosophy of preparing and being proactive and applying it.
So regardless of whether you’ve had children or not, that’s irrelevant.
The pelvic floor is still the pelvic floor and still faces lots of other influences that
can then can impact function and performance.
But if we take that same mentality and say, if I’m lucky enough to reach midlife, I am
going to go through menopause and there are significant changes that happen in midlife
and beyond.
So how can I prepare for that phase of life and how can I keep training the pelvic floor
to handle all phases that I go through?
JANNINE: Absolutely.
Absolutely.
And so thinking about training the public floor, one of the things that I saw, which is again,
post birth, but you had an article that talked about France, women, French women don’t pee their
pants, and how it’s built in to the French, like, medical postpartum care. And so I think
what I’m trying to do is just paint the picture for women who may be like, “Mm, I don’t want to
do pelvic floor.” How important it is. But also, we’ll get there in terms of telling them how you
you can train your pelvic floor.
So yeah, the French article, how did you come upon that?
Like what the?
KIM: I’ve actually known, I hadn’t really shared it that way,
but it’s something that I’ve been aware of for years and years,
especially when I first was starting out in this field,
I worked primarily with pregnant women and new moms.
Now I work primarily with pre- like
perimenopause and postmenopause women.
But when I was working predominantly in the birth world,
We all knew that and still we have all said, why is this not a global standard?
Why is this not happening everywhere?
And the addition to what I shared, so it is an automatic prescription for somebody who
has given birth.
So if you’ve given birth, you are automatically given this prescription for pelvic floor therapy
postpartum.
That doesn’t mean that if you have to have given birth in order to access that care.
So if you were experiencing incontinence or organ prolapse or had other concerns with
your pelvic health, you can still in France ask your doctor for a prescription for pelvic
floor physical therapy that is also in as part of their funding, their government funded
care.
And just today actually, my previous business partner who is a pelvic floor physical therapist,
she sent me, she was originally practicing in Ontario, Canada.
now move down to Texas. But she sent me, she’s still part of the Ontario Physiotherapy Association,
and she sent me an article to read. I have not gone through the whole thing. But it was basically
the Ontario is putting forward a motion to do what they’re doing in France. So that was like
“Hallelujah,” you know? And so hopefully that will kind of spur things on because when you think
about the costs associated with managing and caring for people with pelvic floor dysfunction,
it is in the government’s best interest to apply some of their funding to that in order to prevent
and to help better manage these. And so that in and of itself is a huge argument from a
financial perspective. And then when you think of quality of life of these people, how many people
suffer for years and years and years and how there increased risks of bone loss and heart
disease and diabetes increase because of the limitations of their pelvic floor. Again,
it’s in the best interest of our health care systems to dedicate some funds to prevention
and restorative therapy with pelvic floor physical therapists.
JANNINE: I couldn’t agree more. I couldn’t agree more. I mean, right now in Tacoma, Washington,
and where I practice. We have six pelvic floor physical therapists and they’re slammed. And so,
you know, all of you guys online are my resources to be like, okay, here’s what we’re doing. And
you know, I think also there’s a huge component with the population being of menopausal age. And
having practiced in the same place for over a decade now, I’ve seen women go through this period.
And I’m kind of kicking myself right because I didn’t know enough.
It wasn’t really brought up to me in school about it.
I only had the luxury of having a public floor physical therapist in my
spa that I owned.
And now she’s in my office now because it’s it’s like, oh my gosh.
KIM: Once you know, once you know, right?
JANNINE: You can’t go back.
Like you can’t see that.
You can’t.
You can’t.
And so with the side of prolapse,
with the side of interstitial cystitis,
I mean, I’m seeing all of these different things.
And so I’m very curious on your end
with the programs you have,
what have you seen to be like the most,
like move the needle the most in terms of a program,
like exercise program and serration
to help either rejuvenate or bring things back
or obviously maintenance to just to give folks
a sense of like, all right,
we’ve been having this trouble for a little bit.
What are we getting into to reboot this?
‘Cause of course I want you guys to do this,
but give folks the background in terms of what it’s looking
like on a daily basis, a maintenance basis, a everything.
KIM: Yeah, just to highlight one thing that you said there
with you didn’t know.
And so as I said, if we take the lens,
if we look at it through the lens of,
well, there’s been a huge amount of education now
about prenatal postpartum.
And still, even I’ve been doing,
that was where I started 19 years ago.
And even actually almost 20 years ago now,
when I think about it, but the,
I look at now and say, well, everybody must know
that we should prepare the pelvic floor for birth,
but still it is still definitely underserved.
However, there was a lot more awareness created about it.
So what is happening now with menopause is the world,
the conversation has exploded,
celebrities are talking, everybody’s talking about menopause.
And a component of menopause and the symptoms,
they list off all the millions of symptoms
that we experience in perimenopause and postmenopause,
is there’s a whole section called
genitourinary syndrome of menopause.
And that is all pelvic health, vaginal health related.
So indirectly, the conversation around pelvic health
has been increasing because of this conversation
around menopause.
But to your point, and I am gonna answer your question
with regards to programs, but to your point about,
I didn’t know, but we should be teaching this in schools.
When we teach kids, when I saw that childbirth
education video, I started learning about menstrual health
and about body health, and really it was about
contraception and the period, but even then it was just like,
you’re gonna have a period, and then this is what you use.
Didn’t really tell us about the hormones or the cycle
and what it all means, and that it’s part of this,
you know, our anatomy, this other group of muscles
very close to the uterus that we’re just talking about,
deserves a lot of attention because we menstruate,
because the majority of us are pregnant,
because if we reach midlife, we will go through menopause
and we have all these influences that can create challenges.
So really, this should be taught to our teens
and plant the seed pelvic floor physical therapy.
So what moves the needle the most?
I mean, always my number one recommendation is if you take one thing away from this conversation,
it would be to see a pelvic floor physical therapist once a year, just like you see a
dentist for your teeth for a checkup.
And so just by going to that appointment is not necessarily like I don’t want to say
that’s going to move your needle.
You have to take action with what you learn and what they assess and tell you about your
pelvic floor.
In terms of programs, most people think of pelvic floor exercise if they even use that
terminology or if they think about, “I need something to fix my incontinence.”
They think of kegels.
So Dr. Arnold Keagle, Keagle, Keagle, Keagle, tomato tomatoes, he saw his patients, excuse
me, postpartum who were experiencing more challenges activating and relaxing your pelvic
chlorines experiencing some symptoms.
So he used this device called a perineometer,
which was a biofeedback device,
had some similar properties to this epineo I was talking about,
that helped women see when they were contracting
and relaxing this group of muscles,
that again, we can’t go to the mirror
and flex our pubic oxygias muscles, right?
So this biofeedback device was helping them learn
to contract and relax their muscles.
And then he would send them home
with that new knowledge and awareness,
and now go do sets and reps
of this contract and relax.
So that became a Kegel exercise.
What has happened with the Kegel,
is the Kegel hasn’t necessarily,
it’s evolved in some people’s practices,
but most people just hear the word Kegel
and they think that’s the only thing we’ve got.
And because people are never taught or evaluated,
a PAP once a year or even once every couple of years
is not a real true pelvic floor evaluation.
And so we’ve never really been taught how to do a Kegel.
And so we have pamphlets that have been given to us.
We might have Googled it if it’s been in the last 20 years
or, and so that’s what we do go on.
And we have research to show that the majority of people
actually do them incorrectly
because we have never been taught properly.
So then they go, oh, I tried Kegels and they don’t work.
But Kegels, when done correctly, when done consistently,
are we have loads of evidence to support
that they work very well.
Where I always thought the research and the application
that way fell a little bit short was,
if I said to somebody, do three sets of 10, 10 second hold
Kegels three times a day,
which is what some of the evidence will tell you to do,
that will help, but most people would do them seated
or lying down.
Some people do them at every red light
or while they’re brushing their teeth.
And if it’s done correctly and consistently,
that’s better than nothing.
However, that person may still experience leaks
when they do jumps, box jumps or run or cough or sneeze
because there’s an element of reaction time
that we’re missing out on training
and there’s an element of dynamic movement
and loading that we’re missing out on.
And so my approach has always been let’s take this evidence-based exercise, the Kegel,
and let’s bring it, I call it the core breath because I wanted people to understand that the
pelvic floor works in coordination with the diaphragm and that it is the foundation of the core.
We’ve all heard of core exercise but the pelvic floor has been left out of that conversation.
So let’s take this core breath and coordinate that into full body movement.
And so that’s always been my approach.
And thankfully now there’s research that supports my bias.
And there was two separate studies that I referenced.
One was showing Kegel’s done prior to a resistance training
program.
And another one was Kegel’s done as part of a resistance
training program.
One was in an elderly population even.
And it was showing quicker results and more effective
than Kegel’s alone.
So to answer your question, that was a very long,
winded way back to what has moved the needle the most.
When people understand the connection
of the breath and the pelvic floor
and coordinate that into whole body movement
and progressively load it,
I would say that changes the needle the most on incontinence.
And I would say hypopressives,
which is a whole other exercise technique,
moves the needle the most on prolapse.
And the two together I call the power couple
of pelvic floor fitness.
JANNINE: Wow.
Cool stuff, cool stuff.
I mean, I’m looking at it, right?
I’m 46 as of the time of this podcast right now.
You know what I’m thinking to myself, okay?
I was doing some of the exercises
that have seen with Dr. Bri.
I added a min and I’m like, okay, cool.
I didn’t have any symptoms.
This is where I went wrong.
I was like, yeah, they’re fine.
You know, I’ve been adding it in here and there,
but then I’m not consistent.
And I think that’s where a lot of people will get hung up
like, well, I don’t really have that many symptoms.
or they’ll be like, I do have symptoms,
but I don’t know if it’s gone that far
and that’s where one of my patients was at,
especially with the prolapse kind of situation.
And so having those two dynamic ones
that you’re talking about,
what did you call, I was calling it dynamic duo in my head.
That’s what I said.
KIM: I said power a couple.
JANNINE: Power a couple.
And is now these two, are they part of one of your programs?
Are they part of Buffmup?
Are they part of?
KIM: Yeah.
So the, I originally in 20, I think it was 2017, I created an online program called,
I called it Kegelmojo. And, and you know, lots of people, not everybody, this is before the pandemic,
pandemic, everybody was putting something online. But this was before, so there was enough,
but there wasn’t really an online program. Bri had created one, I think, and at that time.
Anyway, so I created this program and it was self-directed. And, you know, I was thinking,
and of course it’s gonna change the world,
and everybody’s gonna use it and it’s gonna be great.
And it was great, but it was just,
people needed more direction in terms of how to apply
the information to the movement.
So I did provide some exercise and some routines,
but they wanted a bit more structure and handholding.
So I created a 28 day challenge.
There was a company out of Montreal who had created,
they had an app platform that was allowing,
Their target market was fitness coaches,
and they wanted people who were coaches
who were running challenges to use their platform.
So I was one of their first customers,
and I had always wanted an app,
but an app, it’s super expensive
to have your own custom app.
So they had already this platform,
and you just needed to kind of plug and play your information.
So I create this 28 day challenge,
and it took off, like people loved this,
and then I would just run it every month,
And then I’d say, okay, it’s time to buff your muff.
And it just kind of came out as a joke.
And then everyone was like, oh, how buff your muff?
I love it.
And so then I thought, all right,
I’m just going to call it the Buff Muff Challenge.
So originally it was just this 28 day Buff Muff Challenge.
And then I wanted to, like again, people would come in
and then they would want this next step.
Like, now what do I do?
And so it needed to be, I needed to keep people progressing.
And so it’s kind of, it’s this method.
And I do have a membership around it.
And people can use the app if they want
they can use, they can log in online. Not everybody likes to use their phones. So you have options
in terms of how you log in. But it’s very much a lifestyle education. It’s not just, here’s,
do these exercises and everything’s going to be fine. And some people will come in
initially and they go, “When am I going to get to the exercise?” Because there’s about an hour of
content broken into little videos. But there’s about an hour of stuff that people have to go through
first. And I, some people, you know, you could skip ahead if you want to, but you have to
know the fundamentals. You can’t just skip ahead and just like, I’ll just do this exercise
and everything to be fine. You have to understand why the exercise works and what’s contributing
to your symptoms. So I lay the foundation. And one of the other things that a lot of
people, one of the most common comments I get actually is people saying, I’m sleeping
through the night again without having to wake up multiple times a night to pee, which
tell me about life-changing.
When you sleep better, your pelvic health is indirectly going to be better as well, but
so is all the other parts.
Everything is better when you sleep well.
JANNINE: Oh my gosh.
I mean, sleep is such a thing, right?
And being in my side of things, I’m kind of on the bioidentical hormones.
I’m trying to optimize cortisol, things of that nature.
I never thought about the pelvic floor for sleep.
All night.
KIM: Yep.
Yep.
JANNINE: You blow my mind.
KIM: Yeah, and the hormone piece is that will move the needle for some people as well too.
It’s all, it’s, it’s kind of like Kegal’s are not the answer for everybody.
There are multi, there’s, it’s a multifaceted part of the body.
There’s multiple influences that can come in and, and might be a contributor to symptoms
for some people.
And so bioidentical hormones, vaginal estrogen is something I talk a lot about.
I’ve written a lengthy article about that with the evidence as well as part of.
So using vaginal estrogen is not going to magically solve your prolapse or your incontinence,
but it’s going to help.
And then you’ve got the exercise piece.
And then you have the let’s avoid constipation piece that stay hydrated piece.
like, we don’t realize all the things we do, like stop drinking as much water because I
don’t want to leak or I don’t want to have the urges that I’m doing.
And we end up becoming dehydrated, which then the bladder signals you more frequently
to get it out because it’s irritating when you have concentrated urine.
So we think we’re helping, but we’re ending up creating other issues.
Constipation is a major contributor to incontinence and urgency and frequency.
So when people get their bowels moving, yes, that helps to pelvic floor because you’re
not going to strain.
Yes, it helps your incontinence.
Yes, it’s going to help with all of the other things in life because we don’t want to be
cranky-pated all day long, right?
So it’s not just do your kegels and it’s not just a couple of exercises.
It really is a whole body approach.
JANNINE: A whole system.
That’s huge.
It’s huge.
And I mean, just thinking about the hormone situation because I think a lot of people do
think if I just use the hormones.
It’s gonna solve the problem and and yes, I’ve been in that category of trying to explain that’s not the whole situation
You know with the pelvic floor
I’m like thinking about you know a lot of women and I don’t know how much you’ve seen this
But I’m guessing you have because it’s what you do
women that have had the meshes that have had the different lifts the slings things of that nature
What kind of impact does that have on the pelvic floor?
In that case.
KIM: If you think of any surgery, a surgical intervention,
so the mesh surgeries or bladder sling surgeries,
for a while there was mesh use for prolapse,
which the mesh that created the whole scandal
around pelvic challenges is no longer used,
that there is still mesh that is used in the pelvic floor,
It’s just not that same mesh, to be clear.
However, the surgical intervention can be life-changing,
can be an absolutely fantastic option.
It is never what I would recommend
as a first line of defense.
And unfortunately, many people are sent down that path
without looking at all of the other root causes,
basically, for their problem.
And for some people, they have a surgery
it and it fixes the problem, great. For some people it fixes it for a period of time and
then they’re frustrated. For some people it fixes that first problem but now it’s created another
problem and it can become this vicious cycle and people will often come to me and say, “Well,
I’ve had the mesh surgery or I’ve had a prolapse repair, will this still help me?”
And I argue it’s even more essential after surgery. So now coming back full circle to where we started
prevention. If surgery is something we are choosing or is something we need, we need to prepare for
that surgery. We need to train our pelvic floor. We need to prepare our body to undergo that
controlled trauma. And we need to prepare for the recovery afterwards. So we are supporting
the healing process. Then we need like postpartum, we need to retrain that system, the pelvic floor
as part of the core, working with the breath, and then progressively loaded.
And so many people are suffering for many years, finally get so bad they go to the doctor,
and I want to lump every doctor, but this is very, very common I hear it every day.
My doctor said I need surgery, they get referred to a specialist, they’re booked for surgery,
their symptoms are gone initially, and they’re like, “Okay, great.”
But the root causes that contributed to that problem developing in the first place are
many and have not all been addressed.
And oftentimes it seems like constipation, low estrogen,
or lifting technique, repetitive, like all of these things.
And if they go back now with a group of muscles
that has undergone this controlled trauma
that now has scar tissue that can hinder function,
then they’re just going to see a repeat.
And that’s why there is quite a high recurrence rate
of issues post pelvic surgery
because we haven’t looked at all of those things
that maybe could have even prevented that surgery
from happening in the first place, if people knew.
And I’m gonna lump hysterectomies in there as well
because hysterectomy is one of the most common surgeries
performed 600,000 in the United States alone
every single year, often for benign conditions.
And one of those conditions is pelvic organ prolapse.
And if you have hysterectomy for any reason,
it increases your risk of other types of prolapse,
especially the posterior compartment,
which is something called erectosceal.
And if the reason you had the hysterectomy
was because of prolapse, that risk is even greater.
And nobody is told that.
And again, when we think about we need to be proactive
and train the body and recover
and progressively load and retrain that system,
that is absolutely not happening with hysterectomy.
So women are initially like,
“Great, whatever symptoms they had are gone.”
And then several years later,
And now they have other issues that are now further complicated by the fact that there
has been a surgery already.
JANNINE: I see that too.
I see that too.
Yeah, over and over again.
Especially, rectus heels are interesting and fecal incontinence and things of that nature.
Some of the things that women will, like I have to drag it out of people to know that
is…
Yeah, I mean, embarrassing.
I get it.
I get it.
Let’s talk a little bit about that too,
just in terms of the rectum,
in terms of how that plays in to the pelvic floor.
‘Cause I think a lot of people think pelvic floor
and they don’t attach, we’re thinking vaginal area,
we’re thinking female parts,
we’re not thinking about the rectum for some reason.
KIM: Yeah, we think about leaking pea.
That’s kind of what we think about with pelvic floor issues.
And statistically, if you look statistically,
It’s like 40-ish percent are the statistics
for urinary incontinence.
I argue it’s a lot more because there’s a lot of people
who just think that it’s normal and they have to put up
with them, they don’t talk about it with their doctors.
So I think that member is much higher.
Then we look at prolapse statistically.
50% of women who’ve given birth will have some degree
of prolapse in their life and never screen for,
never talked about and so early stage prolapse
is often asymptomatic and so it’s not until it becomes
major problem and it’s probably been developing years and years, you know, over a number of
years.
And people are really sidelined, but that’s a bigger percentage of the population.
And often they’ll have incontinence and pelvic organ prolapse.
And nobody’s heard the term prolapse before.
It’s starting to become talked about it a little bit more now, but nobody’s really told
it.
And if you look sometimes even in the literature, prolapse is more historically, I would say
this is.
It’s always just the womb prolapse or the uterus prolapse.
If the bladder and the rectum were never considered as something that could prolapse,
it was always just the uterus.
But rectus seals are really quite common.
In pelvic organ prolapse, what’s happening is the bladder, the uterus, and/or the rectum,
sometimes even the intestines, will shift out of their optimal anatomical position and
start to bulge into or descend into the vagina.
Early stage can be asymptomatic as it becomes a bit more advanced.
Some of the more common symptoms would be low back pain, sense of heaviness or dragging,
feeling like something’s inside your vagina, difficulty with insertion, difficulty starting
the flow of urine or feeling like you don’t empty, urinary tract infections, difficulty
emptying the bowel, always feeling there’s something like stuck there bulges.
So if it becomes more advanced, you may see or feel a bulge at the opening of the vagina.
In extreme cases, it bulges outside.
It almost looks like a scrotum to some extent.
And it’s very, very life altering.
And the recticeal in particular, I’ve experienced all of them.
I’ve had a Stage 2 uterine prolapse.
I’ve had a Stage 2 recticeal.
Right now I have a very early stage ladder prolapse that’s been there for a long time
and it’s just kind of hanging out.
Didn’t mean it to say like hanging out,
but just there.
But the so the uterine prolapse was what presented itself first.
During my perimenopause transition,
I didn’t know the term perimenopause.
I had no idea what was happening with me.
Constipation was all of a sudden something
I was dealing with I’d never had before in my life.
Never changed anything.
I ended up having an underlying autoimmune condition as well.
as well, how she modals.
But once I figured all that out,
it was, I’d been straining quite a bit.
And my uterus was just one day I was having sex
with my husband and all of a sudden it felt like he hit
something and it was sort of jarring.
And I went to my physio who I’d seen about six months earlier
and she’s like, yeah, your uterus is moving south.
And so with hypopressors, and I was already doing buff muff,
but it was right around that time.
Thankfully, I had learned hypopressors
and started applying that.
And I was able within a few months to reverse that.
I’d also had an early stage recto seal
that continued, like it didn’t progress terribly,
but it just over time would continue
to progress a little bit.
And it became symptomatic.
And I did all the things.
I threw everything, the kitchen sink at it.
And after nine years, I just said,
there’s nothing more that I can do here.
And I’m tired.
These symptoms are interfering with the quality of my life.
I chose to have surgery for that. At the time, I did, again, I have an early stage bladder
prolapse, but I chose just to leave that as it is. And so I had a posterior recticil,
well, posterior vaginal wall or a recticil or a pair at three and a half years ago,
December 2020. And that opened up that, like, I felt like the biggest hypocrite. Here I
am telling everybody how to avoid surgery and deal with these exercises. But it was also
So it’s a moment where you realize exercise won’t fix everything hormones won’t fix everything
avoiding constipation won’t fix everything sometimes there is damage to the tissues for
whatever reason I then found out just before I had my surgery so that was 14 years after
my second birth that I went to a new physio and she suspected I had something called a
levator avulsion which is a where part of the pelvic floor is not attached to the bone
anymore. And this actually happens in about 30% of vaginal births. Again, not screen for,
nobody knows. And so I still went ahead with the surgery. And it was just about
eight months ago, I can’t remember exactly when, but eight months ago where I actually
fit like had it confirmed with 3D ultrasound with a position that I have that. So that
increases my risk for prolapse and all the incontinence and all the things. But one
common comment he made was, it’s really good that you have been so consistent with your
pelvic floor exercise because the muscles that are intact are all very, they’re doing
the job very, very well, even though they have to compensate for that challenge.
So anyway, lots of things were kind of working against me and there was no, all the exercise
in the world, all the hormones in the world were not going to fix my rectus ill, so I
chose surgery at that point.
But I prepared for it.
I trained for it.
I did all the things to get myself in the best state possible.
I had a full recovery protocol.
I did progressive loading.
It wasn’t until six months post-op where I was back to loading like I was before.
And it became a new program, actually, oddly enough, because I said, like, there’s no
support for people going through pelvic surgery.
I really want to highlight that surgery can fix symptoms, but it does not fix root causes
and it does not just magically optimize your function.
It can help improve anatomy, which can help improve function, but you still need to do
the work to get the muscles working well again.
JANNINE: I’m speechless.
I’m like, holy cow.
I never knew that you could tear the levator.
Is this levator Ani?
I’m guessing, yes?
KIM: The levator ani, which is a group of muscles,
and it’s one part of the pelvic floor.
And it is, yeah, an avulsion injury.
The terminology is–
JANNINE: Pulled off the bone.
KIM: Right
Yes, and you can have a partial,
or you can have a full, you could have one side,
you could have bilateral.
And so mine is one side on the left,
and he said there was one little section on the right,
But he said I wouldn’t even really, you know, it wasn’t a major issue.
It’s more of on the left hand side.
So two, two muscles, two of my levator muscles are not attached.
JANNINE: I had no idea.
This kind of thing had happened.
And, and now the thing, I’m like, okay, how can we help some folks to maybe
clue in that this could be a thing and, and like see if they could get
someone to do a public ultrasound to find it.
Like, is it a transvaginal ultrasound that finds these kinds of things?
Or I mean, I’m imagining you need somebody that knows
that this can happen because–
KIM: Yeah, so right now, and again, I live in Canada
and the person I went to go see is in the United States.
And the reason I went to him was he was actually,
I had invited him on my podcast
to talk about levator avulsion.
I’ve had a guest on my podcast who is an advocate.
She has had suffered tremendously with bilateral avulsion
and has been an incredible advocate
for this population of people.
And so I’ve had her story and then after my physio
just before my surgery had said,
“You know, I think you have one.”
And it had always just kind of been sitting there in my mind.
So I brought this doctor on ’cause he is one of the only
people who have surgical techniques to repair.
So historically up until now it’s really been like,
well, there’s nothing we can do.
There’s no surgical repair for an avulsion injury.
And he is using new techniques to change that mentality
and has really helped bring people’s quality of life back
as much as possible.
So I had him on the podcast, and then he’s in Washington, DC.
He said, well, if you’re ever here,
let’s check it out and see.
We’ll confirm it.
So I made the decision to go and say, all right,
if I stay in Canada, it will probably take me maybe a year,
year and a half to get the requisition to get the imaging to go and I’ll pay the money.
Anyway, I did it.
It was almost like a pelvic ultrasound, so a wand that’s inserted and he rotates around.
I was watching, I filmed it, I will be sharing some of the images of the time I wanted to
film the whole thing.
It’s long, so I won’t share the whole thing, but just little snippets of things that he
He has said in images where you can see the deficits compared to the healthy attached
muscle.
JANNINE: Wow.
Yeah.
That’s crazy.
I know no idea.
No idea.
KIM: Yeah.
And it’s, you know, if you look at research, 30%.
And they say that, like, it’s a word, like minimal of all of them, there can be some
recovery over a period of time, but especially the really significant injuries. There’s
currently nothing. So there’s no screening in place for that. There’s nothing that says,
well, if we could intervene with these protocols, maybe it would help a little bit.
So many people are walking around with a volumine that have no idea. And so if you have tried all
the things for six to 12 months, seeing pelvic floor physical therapy, you’ve done the exercise
consistently, your technique is good. You’ve tried hyperpresses. All the things and nothing
is moving the needle, then it’s worth, and not a lot of manual pelvic floor therapists,
you really need imagery, you need imaging to confirm it. Some of them may use a transparinial
ultrasound, but you need more than that, like MRI even. And so many physios, if they’re even
feeling and assessing for it, they couldn’t diagnose it. They could say, I suspect it,
but the people would then themselves have to go and ask for imaging to confirm that,
and that can be a long process.
JANNINE: Ah, oh my goodness. So in my mind, of course, I’m going, okay, child birth one way to have
an avulsion. Is there any other way like say someone had a really bad skiing accident yard sale
one leg’s going this way the other one’s going that way like I’m thinking spread injuries or I’m
thinking like something’s in the case of skiing and I’m going to explain myself for a moment because
you got my mind going a little bit about does this make sense? I don’t do well with deadlifts
And I always feel like a tearing pain, very deep,
very on the ins, like where the levator,
and I would attach to my right side of my pelvis, basically.
And so I’m like, okay,
’cause I’ve had overstretch injures
where I literally almost did the splits
with one ski going one ’cause it got stuck
and the other one keep and goin’.
Does that kind of situation preclude to you?
KIM: You know what?
I have thought of something like that too.
And I’ve never looked, and I’m gonna do it now.
I’m going to look in the research.
I don’t know of all the research I’ve done looking at pelvic floor or even just
a vulture.
And I’ve never seen any reference to anything other than childbirth, but I could imagine
a car accident with certain, you know, very sudden tearing motions of like limbs going
different ways and ski for sure.
I bet you.
I just don’t know if there’s anything published on that, but I’ll look and I’ll get back to you.
JANNINE:I look forward to seeing that.
I’m kind of, I mean, I’m just, I’ve been trying for like most of my life to figure out why I have this weird tearing pain.
In my way.
KIM: Have you seen a pelvic floor physical therapist?
JANNINE: I have and nobody has noticed anything.
And granted, it’s been a couple of years because this, this started like over a decade ago after
this injury.
And, and at the time when I first had someone look at it, I’m wondering if maybe, maybe my tissue wasn’t inflamed.
I don’t know.
I don’t know.
That’s a good question.
KIM: Yeah, and it would be, I would,
many therapists will assess in different positions as well,
like, operate against gravity and trying,
so for you, I would think, I don’t know what your,
how your injury happened, your saying skiiing.
So I’m imagining there was a, like you say,
there was a spread.
So if you were, I’m just thinking,
if you were a patient and I was doing
an internally evaluation, I would take the limb
try to move it through ranges of motion to try to replicate that stretch
Sensation that you feel in a movement or you said a deadlift is where you feel it
So I would even assess like me as the therapist. I am not an internal therapist
But if I was I would be on the floor
I would have my fingers inserted and I would have you do the motion of a deadlift to try to replicate that sensation
even if it wasn’t if you’re not under load it might not happen as much but and
And see if we can see is it does does the muscle function differently?
Is there something that’s not moving accurately?
Is there a pull?
Is it right?
So maybe it’s not an avulsion.
Maybe it’s simply there was some disruption, but there’s maybe some scar tissue
that’s still residual there.
But I’d want to try to see if we could find it through movement.
JANNINE: Makes sense.
Makes sense.
Gosh, there’s so many things with the pelvic floor that I could go down.
You know, rabbit holes, like you’re saying with the motion under load, different,
different movements. But yeah, I will definitely look into that.
Cause now that I’m learning these things, I’m like, when that, I mean,
the way that injury happened was insane. And so, and the pain was pretty bad.
So I’m like, and I haven’t been right since. Let’s put it that way.
But it’s something to think about. And I just bring up guys for the podcast
just for you guys, if you’ve ever had something, you know, where it just
haven’t been right since. Yeah, that’s important. The other big thing that I’d love to chat about
before we wrap things up is talking about vaginal health because your podcast title between two
lips, love it, love it. It’s good stuff. It’s good stuff. There’s so much that happens between the
two lips that as we get older and as I am seeing more and more patients, I am, let’s say increasingly
horrified that we’re not talking about this as much to the point where I’ve had some patients
where their two lips were sealed together because of that much inflammation. So tell us a little bit
about how you help folks in that department, what you’ve seen to be beneficial, what’s your
insider scoop in that department, what should we all be thinking about who are preventative
and maintenance.
KIM: Yeah. The term that I referenced early, Genito urinary syndrome of menopause,
GSM, used to be called vaginal atrophy. And the terminology was not representative
or didn’t represent all of the different symptoms that somebody could be experiencing
as it pertains to their vaudevotional health. And so the word syndrome indicates a collection
of signs and symptoms, and we can have genital symptoms, we can have urinary symptoms, we can
have sexual symptoms, and so different things will fall under each of those categories that are
estrogen gets the blame in terms of it’s the low estrogen state. That’s why this is happening.
excuse me, and it absolutely plays a role, but there’s so many different things.
There’s age-related muscle loss.
There’s collagen loss.
There’s hyaluronic acid loss.
There’s bone loss, and all of those can play a role in creating or manifesting these symptoms
that we may have in the pelvic region, the whole vaginal health.
So statistically, I’ve seen between 50 and 80% of women will experience some, not necessarily
always all, but often many of the symptoms of GSM.
So 50% is high enough.
If it’s actually even upwards of 80, like that’s a lot of people.
And this is something that we also know does not improve.
It’s not one of the symptoms like, “Oh, your brain fog, it’ll go away.
Oh, your hot flashes, it’ll eventually go away.”
This does not improve with time and will continue to worsen unless addressed.
So knowing that information and knowing also that many of those symptoms, the first, I
don’t want to say always the first sensations, but where they become most bothersome is usually
a few years into the postmenopause period.
So once you’ve reached your one day of menopause and beyond your postmenopause, it’s usually
a couple, two to three years afterwards, whereas things are starting to get bothersome. So knowing
that, maybe we could be preventive. Maybe we could say, let’s intervene. Like, as I’m hitting my menopause,
one of the things that I’m now going to do to support my pelvic and vulva vaginal health is to
use vaginal estrogen. Vaginal moisturizers play a role. I argue things like collagen and creatine
and vitamin D and C, buckthornyl,
off from a supplement perspective also play a role.
But vaginal estrogen in particular,
it will help all of those symptoms.
But one of the main reasons is the reduction of UTIs.
So the increased likelihood of UTI urinary tract infection,
skyrockets, post-menopause, especially
due to that low estrogen state that now changes
the pH of the vagina.
So we usually are quite acidic.
that helps us spend off infection.
Without estrogen, we now are, we lose that.
The pH has changed, less acidic,
more prone to infection, UTIs.
People get treated multiple times for UTIs
and then it becomes resistant
and now no antibiotic is going to work
and that can become life-threatening.
So if it is only for reduction of the risk of UTIs,
that is motivation enough for me.
But it also will help with painful sex, dryness,
burning, irritation, urinary frequency, urinary incontinence,
urgency.
You mentioned the labia of your client.
We, everybody’s got different sizes and shapes,
but we have this plumpness and juiciness in our tissues
that loss of estrogen and the loss of, you know,
all the other things that are saying hyaluronic acid
and muscle loss, what have you,
the term atrophy is essentially a shrinking or a drying or thinning of the tissues.
And when left untreated, the opening of the vagina can close.
The labia can retract and as you say, they just sort of almost like they’re fusing together in a sense.
And it can happen around the clitoris.
Like it can, it’s drastic how it can alter the appearance and especially the function
and the feel of our tissues.
So again, I’m always kind of thinking of this, what can we do to prevent this?
If we know this is a huge risk, I don’t want to wait for symptoms.
What can I do now to help prepare?
And there is loads and loads and loads of evidence about vaginal estrogen and people
always are very afraid of the word estrogen now because of the Women’s Health Initiative.
And I shared a bunch of research in an article.
There’s oodles and oodles and oodles and oodles of research now to show that if anything,
it decreases our risk of many different types of cancers.
And there’s no increased risk for mortality or recurrence in people who have had, in particular,
breast cancer is a big one that people are concerned about when using vaginal estrogen.
So I say it’s not a nutrient, but I jokingly say it’s like an essential nutrient.
JANNINE: Yeah.
Yeah.
I absolutely agree with you.
I absolutely agree with you and I, women’s health initiative study.
Oh.
KIM: Yeah.
I know it created a big, it’s maddening.
It’s maddening when you know the, when you know the history and the story and the misrepentatation
of data and the way the media, Dr. Kelly Kasperson shared an incredible podcast episode called
Boomers Should Be Pissed.
And that says it, like a whole whole generation missed out on incredibly beneficial therapies
because of the misrepresentation of data from that study.
Now, we’ve also learned a lot from that study, but went that initial headline that was not
accurate and then all of the follow up positive things have never been shared with the same
vigor and, you know, publication. So there’s a lot of people working very hard to make things
viral on social media. And the word is starting to get around, but there still is this, like,
I think, keep thinking, people must know that now, but no, every day I’m asked about breast cancer
or an estrogen.
JANNINE: Me as well.
Me as well.
No, it’s still, it’s still there.
The fear is real and I mean, even on social when I post on Instagram, there’s always going
to be haters in there being like, you’re making people get cancer.
KIM: Oh, I know.
I know.
Yeah.
We just have to share the research.
JANNINE: Like go eat your Cheetos and hang out in your mom’s basement.
Seriously, stop, stop.
You don’t even know.
KIM: Yeah.
JANNINE: But yes, I mean, the research, the, the roof, right?
now we’re starting to have women who have done the bioidenticals. Like I have some women in my
practice who are in their 80s and have been on bioidenticals since their 50s. And I’m seeing how
amazing they look and vibrant. And so I hope that is the proof for folks to turn this around that
we can definitely use that. But gosh, just knowing all this information, like, can you have
I’m like, oh my mind on so many things I had no idea about,
no idea about.
And I’m like, why?
Like, same like you, why are we not teaching this
in grade school?
Why is there sex education class not about that
versus scaring the pants off you about getting pregnant?
KIM: Yeah.
And also fitness education.
I know what I know we’re wrapping up,
but just one final point.
JANNINE: No, go for it.
KIM: Fitness education.
If I’m responsible for moving people’s bodies
and improving muscle function,
I should know about this other part of the body
called the pelvic floor, which is a group of muscles
with type two and type one muscle fibers and has a type,
like all the other parts of the body I learn about how
to contract and which exercises are best,
that should be fundamental in anybody who’s taking
fitness and movement, like becoming a personal trainer
or a fitness instructor or movement therapist,
whatever it, the pelvic floor needs to be in that base.
It shouldn’t have to be as it exists now,
continuing education, that should be base level knowledge
in those certifications.
JANNINE: I’m in a hundred percent agreement with you
because I’ve not, you know, in my different programs
that I’ve been through with fitness,
there hasn’t been anything.
And, you know, only because of you and Dr. Bri,
did I even figure out in addition to the gals in my office,
that I should probably be thinking about this
with my lifting, because, you know, with power lifting,
it’s heavy weights, it’s a lot of load on the body.
I love the daylights out of it,
but it’s, I’m certain I might’ve had like four children
children with the amount of load that I’ve put on my I don’t know, right?
I don’t know.
But these are the things that it’s so important for folks to be taking away
and especially with fitness because I think a lot of women I’ve talked to over
the years have been like, I can’t go to the gym.
You know, I can’t like if they make me do burpees or jumping jacks, you know?
KIM: Yeah.
Right.
Yeah.
And that’s a signal the body is sending you saying, I need some help here.
It doesn’t mean that you can’t ever do that exercise again.
It just means that currently I need some help, but let’s rebuild it.
And people can lift heavier and can last longer and can perform exercise better when their
pelvic floor is optimized.
But so many people stop exercising or told they can’t do certain things or just self-select
out of certain movements because of these symptoms.
But we, we, it doesn’t mean that that exercise is bad and there isn’t a safe and unsafe
list.
It’s just a, let’s check your execution, let’s check your strategy, let’s build the capacity
in your pelvic floor.
would build any other part of the body to manage a heavier load.
JANNINE: Absolutely.
Oh my goodness, such stage advice.
Perhaps you have it in you to create a continuing education program that can be built into
eventually a full scope program for fit.
KIM: Well, I do have a certification.
And I actually have one coming up in San Diego in June.
And it used to be called the core competent specialist certification.
And it’s now in the process of being renamed to just female core and pelvic floor fitness
certification.
JANNINE: Oh, wow.
KIM: Come take it.
JANNINE: Dude, I’m so in on all these things because I mean, it’s like every day in my office,
right?
And so I feel kind of like I’ve, the boomers in my practice should be pissed at me for
not knowing all this information.
But here we are.
I’m trying to make up.
KIM: It’s not your fault.
You didn’t know.
Yep.
JANNINE: Trying. Oh my goodness.
Let’s tell folks where to find you.
Let’s talk about your 28-day challenge,
buff muff everything, and your podcast,
between two lists.
I’ll let you tell everybody everything,
and where to find you.
KIM: Thank you.
I really enjoyed this chat,
and I really appreciate the opportunity to share,
so thank you.
My website is vaginacoach.com,
and if you go to Google and put vagina coach,
you’ll find me on some platform.
And through there, you can find the link to my podcast,
which is Between Two Lips.
You can find my blog where I share all sorts of different articles.
You can also find the link to Buff Muff.
So you can also go to BuffMuff.com.
People basically come in and start with the Buff Muff method.
It’s $17.
And in that, they get a free gift of the $28 due challenge as well.
So it’s a very comprehensive program for $17 and lays the foundation.
It gives you everything you need.
If people want more with coaching and more workouts and, you know, kind of progressing
beyond there, they can come and join the membership if they like, but you can just do the one
time payment of 17 bucks and you get everything you need, including the challenge one time
and you’ll be off to the races.
JANNINE: I love it and so cost effective.
My goodness.
All right, guys, don’t, don’t, don’t wait another day.
Literally do not do that.
Please, please take care of your pelvic health.
It’s going to be so much better.
I mean, God, we have these commercials on TV that just make me want to cry.
The wick thing and the, no one wants that.
No one wants that.
So.
KIM: And it’s not just part of being a woman.
JANNINE: Amen to that.
Amen to that.
It is not normal, not part of being a woman.
Guys, you got stuff you can do.
And Kim’s got you covered.
Thanks again for coming on.
I appreciate it.
KIM: Thank you for having me.
Hey, health junkies
Thank you so much for listening to another episode of the Health Fix Podcast.
To help support my mission, to bring you tips, tricks, and tools to help you optimize your
health, I’d be grateful if you’d like, subscribe, and write me a review for the podcast.
And if you hear a product you’re interested in on the podcast, you can now go over to
my website to learn more.
That’s Dr. spelled out, J-K-R-A-U-S-E-N-D.com.
click on shop and you’ll find all the information on my favorite products that I stay behind and
use myself. All affiliate income earned with your purchases goes directly to help support the
production of the podcast so I can keep bringing you quality health information. I appreciate your
support and I’m honored to have you listening to my podcast as a fellow health junkie. Thanks again.
Hey fellow health junkie, thanks for listening to the HealthFix podcast. If you enjoyed tuning in,
please help support me to get the word out about the podcast. Subscribe, rate, and review,
and just get that word out. Thanks again for listening.