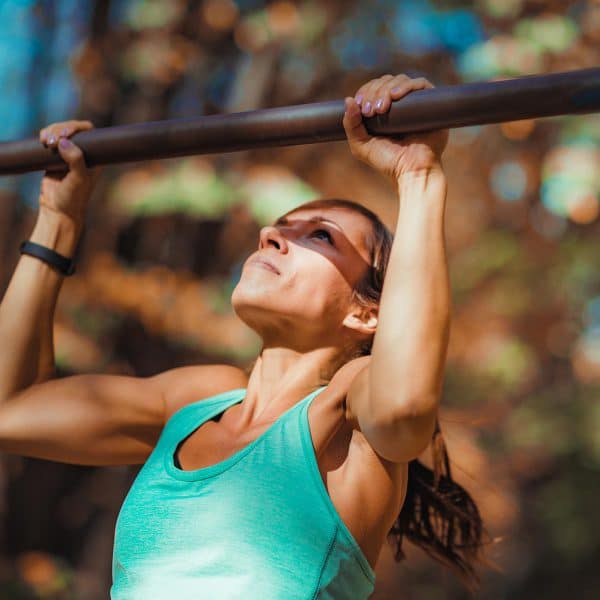
Did you know your mouth is a mirror of your overall health?
In today’s episode, holistic dentist Dr. Michelle Jorgensen joins Dr. Krause to uncover the hidden connections between your oral health and chronic conditions like fatigue, hormone imbalance, and even cancer risk.
A former traditional dentist, Dr. Jorgensen’s own battle with mercury toxicity changed the course of her life and practice. Now she helps patients heal at the cellular level by starting where true health begins: the mouth.
If you’re tired of chasing health trends and still not feeling better, this episode will help you uncover the root causes you might be missing.
Dr. Krause’s Protocols
Instructions Included
Traveling soon? Looking to detox or reset your gut? Try one of Dr. Krause’s Fullscript plans.


🔍 What You’ll Learn
- Mercury Toxicity: How Dr. Jorgensen discovered she was being poisoned by her own practice
- Hidden Dental Infections: What they are, how to detect them, and why they can sabotage your health
- Cavitations & Cancer: What’s the link and when to investigate
- Airway & Sleep: How your bite and jaw alignment affect sleep apnea and energy
- Hormones & Teeth: Why gum recession may be a hormone issue—not just a brushing problem
- Wisdom Teeth Done Right: Ozone therapy, PRF (Platelet-Rich Fibrin), and biocompatible protocols
- Preventive Dental Care: Nutrition, oral hygiene, and the real daily practices that matter
- Emergency Tooth Tips: What to do when you feel soreness, sensitivity, or chip a tooth
- Homestead Living: How Dr. Jorgensen walks her wellness talk on her own homestead
💬 Memorable Sound Bites
🗣️ “Mercury toxicity can stem from dental practices—not just fillings.”
🗣️ “Your mouth tells the story of your overall health.”
🗣️ “Root canals may lead to chronic infections and immune system issues.”
🗣️ “Preventative care includes proper nutrition and daily awareness.”
🧠 Key Takeaways
- Mercury exposure can silently impact your health.
- Hidden dental infections and cavitations can fuel inflammation and fatigue.
- Airway evaluation is essential for sleep and longevity.
- Nutrition + lifestyle = the foundation of true preventive dentistry.
- Holistic tools like ozone therapy and PRF can speed healing and reduce risk.
🩺 About Dr. Michelle Jorgensen
Dr. Jorgensen is the founder of Total Care Dental and Wellness in American Fork, UT, and author of Living Well with Dr. Michelle. A pioneer in holistic dental care, she helps people heal from chronic illness by identifying dental sources of toxicity and teaching how to live vibrantly through natural methods.
Learn more: https://livingwellwithdrmichelle.com
Our Partners



Podcast Transcript
Jannine Krause (00:01.103)
Dr. Michelle Jorgensen, welcome to the Health Fix Podcast.
Michelle Jorgensen (00:04.354)
Thank you, I’m excited to be here.
Jannine Krause (00:06.399)
I have been looking forward to this podcast for some months now, since quite a few of my patients have actually said, when are you going to get Dr. Michelle on? Because teeth, you know, it’s a thing. We all have them, hopefully. If we don’t, we’ll talk about that too. But it is something I don’t talk about as much because I am not an expert in the dental realm, but we always talk about how the mouth is so much part of your health. So thank you so much for coming on.
Michelle Jorgensen (00:33.966)
I’m excited to talk about these things because they are important.
Jannine Krause (00:36.837)
They absolutely are. And one of the biggest things that drew me to, but also just was fascinating is the mercury toxicity that you experienced yourself. Because a lot of folks are going to think about it in terms of amalgams, but they don’t think about it in terms of secondary exposure. And I have a lot of patients who are in the dental field. So it’s definitely something that I want to bring some awareness to environment and how things can affect. So what was it like to have mercury toxicity for you? How did you even know that something’s off?
Michelle Jorgensen (01:07.33)
Well, it was an interesting journey. It certainly wasn’t intentional. It wasn’t anything that I could put my finger on for a long time. And you know, before we got on, you talked about people with mystery illnesses. Well, that’s really where I was at. So I was 10 years into practice and you know, busy, really busy practice, four young kids, a lot going on. So I wasn’t feeling well, but I think a lot of times we just write it off as, this is just my life and I’m just stressed out and whatever it might be. But things got worse, not better. And the symptoms were…
gut issues, but it’s interesting with gut issues, everybody just assumes that everybody has them, you know? And what do do? You just throw away all your food and you start over. So that’s what we did, you know, we threw away all of our food and we started over and it helps some, but it didn’t help a lot. So things were still not good. My memory, I’ve always had a good memory and I got to the point where I couldn’t complete sentences. I couldn’t remember patients names from room to room.
So my husband was really concerned because he said, this is not you. You know, I’ve known you a long time. This is not you. But the one that was really debilitating was I had just numb, painful numbness all the way down my arms, my hands. couldn’t sleep at night. I couldn’t blow dry my hair. I couldn’t hold a pen. And it got to the point that I couldn’t even hold my dental instruments. I just didn’t have the dexterity to do it. My hands were completely numb. I would stop and shake my hands in between about every two minutes between doing my work. And I just said, well, I can’t do good work.
if I can’t feel my hands. So I put my practice up for sale because I was seeing doctor after doctor after doctor. People would get, send me home with a prescription. You know, it didn’t help. Like, you know, they put me on like an acid producer medication. I’m like, well, I’m sure that’s going to help a lot. Let’s do that one. So, you know, all of these different things that didn’t help, but they didn’t know what to do with me. No one had answers. So put the practice for sale.
And in the middle of all of that, not knowing what we were gonna do, as in my mid-30s, like I said, four young kids, this was the livelihood for our entire family. My husband worked for the practice as well. We were in really desperate times. And finally, another practitioner just said, you know, have you ever looked into mercury poisoning as a problem? And I said, well, I don’t have fillings because…
Michelle Jorgensen (03:12.416)
Silver fillings are 50 % mercury. They are. So every filling anybody has in their mouth right now that might be silver is 50 % mercury. I knew that. You know, they teach us this in dental school. So I knew that. But I said, well, I don’t have any fillings. He said, it’s not the fillings you have. It’s the ones you’ve been drilling out for the last 10 years with no protection. And that was literally the first time I had ever heard those words or had ever considered this could be a problem. Because in school, what I was taught is that if I told someone that those fillings could affect their health,
I would lose my license. That’s what I was taught. So this was not only not on my radar, it was off my radar because I didn’t want to lose my license. So I said, no, no, no, I’ve been taught they’re completely safe once they’re in the mouth. This is not an issue. And he said, well, isn’t it worth getting tested just to be sure? And I thought, well, yeah, because I’m about to lose my entire livelihood here. Let’s give it a try. Got tested and that’s what it was, mercury toxicity off the charts. So I had no idea.
this could even happen to me. Had no idea this was a thing, had no idea this was a risk for a dental professional, and it wasn’t just me that was at risk, it was everybody sitting in that office. So, you know, it’s the HVAC system circulating all of this. So it’s the dental assistant for sure, the dental hygienist that’s cleaning these teeth, it’s the dental receptionist sitting at the front, it’s everyone that’s getting exposed to this mercury. And so what ended up happening is…
The doctor said, you can’t take it out if you keep putting it in. So somehow you got to figure out how to do this if you’re going to keep your job. So I found an organization that actually had protocol to remove these fillings and not get exposed, both the patient and the practitioner didn’t even know they existed. So I just started doing these protocols and it was very noticeable, you know, as patients would come in and I’m wearing a mercury filtration mask and we’re covering everything in the room, including them. have giant vacuums and they’re like, okay,
it here and so you know I would explain to people well this is for me but then they would usually go well but isn’t this probably better for me too yes actually it is and then they started telling friends I thought it was gonna chase away all of our patients I thought all our patients would quit coming you know because they would think I’m just like crazy town but they started telling people about it and people were like I’ve been hearing about this she’s doing that now okay we started seeing people specifically for this the practice started growing
Michelle Jorgensen (05:34.157)
And then they would send doctors our way, doctors who are looking for practitioners who are doing this. And the doctors would say things like, I know you dentists haven’t trained the fluoride is the only way that you’ve got to do fluoride, but what do you really know about it? And I’d sit there and think, well, well, I know it strengthens teeth, but what do you really know? So then I’d have to go research because that’s the kind of person I am. And then I found the truth. And they’d say, what do you really know about root canals? Well, I’m doing one.
in the next hour, what do you really know about them? And then I’d have to go find the truth and find the answers and the research that supported it. And all of those things just snowballed. So it wasn’t me intentionally looking for these things. It wasn’t me assuming this was mercury that was my problem. It all came because I had an issue, didn’t have an answer, had to find an answer. When I did, I found a whole bunch of other answers I did not expect. So it was certainly not intentional.
Jannine Krause (06:28.889)
man, you know, in a way, I always believe that energetically that was meant to happen so that you can be here today and educating folks and really waking folks up because we’ve had a revolution of waking up in the medical industry that things are not what they seem. Same thing goes for the dental industry. Same thing goes for veterinary interest tree, you know, it’s it’s all we’re starting to realize why we’ve really
And and one of the things that I really love about your practice that I was checking out is the hidden dental Infection exam that you guys offer because I can tell you as a doctor myself. I will send patients to Holistic dentists folks that are calling themselves holistic dentists and I will say hey, I really need a cone beam exam I need it, you know check this tooth blah blah blah And then the patient comes back and says yeah, they said I’m fine and I’m like, well, what did they do? Just an exam. I’m like, did they do any x-rays?
No. Did they ask you about your health? No. So I would love for you to enlighten folks what a real dental, like hidden dental infections exam looks like from your lens and what you guys are up to because I think we’re, we have a lot of people out there, probably well-meaning dentists to, to try to help, but we’re missing some links here.
Michelle Jorgensen (07:45.059)
Yep. And really honestly, my practice evolved. You know, it started with mercury removal and then I learned about infections and then I learned about fluoride. And so I’m hoping that all of these people are in the evolution mode, but it’s, frustrating as a patient because you hear this and you say, well, I want all of it, but your dentist is only on step two of step seven. You know what I mean? And so I’m going to teach you what to ask for on the phone, which will really, I think help alleviate that as well. First thing though, let’s talk about what are these hidden
infections. Which ones are we looking for? So really there’s three main ones that are going to be found in the mouth and one every dentist is going to talk about that’s gum disease.
Jannine Krause (08:15.065)
Yes, absolutely. Yeah.
Michelle Jorgensen (08:23.746)
That’s actually one that we’re all taught how to deal with. We’re all taught how to record and measure in our offices, and we’re all taught how to treat it. Now we do treat it a little differently than perhaps another office does, but every office is going to measure your gums. If they don’t, then they really aren’t actually even practicing standard of care of dentistry. So every office should be measuring your gums, six measurements on every single tooth to see what is the health of the gum and the bone underneath. That’s pretty standard.
You’re gonna find that pretty much in every dental office. And dental gum disease is prevalent. 70 to 75 % of all adults have some degree of gum disease. And gum disease is the most researched dental disease that there is actually. There’s hundreds of research articles showing the connection between gum disease and heart disease and kidney disease and lung problems and low birth weight babies. I mean, it goes on and on and on on on. So at bare minimum, you need to have your gums checked. But that’s not where you should stop.
There’s two other infections that you really need to know about. The first is root canals and the second is where teeth were removed. So let’s dig into those just a little bit. So root canals, what’s the problem?
And this one, like I said, I’ve done hundreds of root canals myself in my career. I didn’t know any of this. So I’m going to teach you kind of the way I learned it. Inside of a tooth, when a root canal is done, what we do is there’s either a cavity or a crack that’s infected the nerve or affected it. You so that’s the toothache. You’re like, my gosh, I drank that thing and it just hurt for like five hours after. I’m driving down the road in my car and what is that? It’s killing me. That means the nerve inside the tooth is
It’s dying. It’s either dying or it’s already dead. So what a root canal is, is the dentist makes a hole in the tooth. You get into that nerve area. So there’s the nerve and the blood vessels on the inside of the tooth.
Michelle Jorgensen (10:08.202)
Clean it out. We use little tiny instruments that we use to clean out that nerve and that blood vessel. Take it all out of there. Sterilize it so it’s disinfected with bleach. Actually, that’s still the material of use. So it’s bleach that we put in there. We let it sit there. People will be like, why does it smell like bleach? Because it’s bleach. So you use bleach because it does kill bugs, OK? So you put bleach inside of the tooth. You let it sit for a bit. Then you fill it up with something called gutta-purcha.
It’s like a rubbery material. If you heat it up, kind of flows and flows into the tooth. So it entombs the tooth in essence. The idea of is it awesome? Like you get to chew with the tooth still, you get to smile with the tooth still. I mean, it’s awesome. It doesn’t hurt anymore because the nerves gone, but that’s not all that’s inside of the tooth. So there are the main nerve canals, main blood vessel canals.
but there are these little things called dentinal tubules that go off of that main canal. And every dentist knows this. We were taught this in first year of dental school. So these dentinal tubules are why when you tap your tooth, you can feel it, right? You tap here, you can feel it because there’s nerve, little nerve extensions that go all the way out to the outside of the tooth. It’s also why cavities spread because cavities get into those little holes in the tooth and then they start to spread deeper into the tooth. It’s also how you get nutrients into your tooth.
You know, you get more minerals in here if they need more minerals, it’s through these little nutrient channels, these little dentinal tubules. They’re too small to clean and they’re too small to fill. Every dentist knows this as well. Otherwise on like an x-ray, we’d see these teeny little fillings going all the way off of a root canal. We never see those. So you always have dead nerve tissue and dead blood vessel tissue left in those tiny little tubes, no matter how well the root canal was done. So at first it’s fine.
Nerves gone, blood vessels are gone, everything’s great. But that dead tissue is gonna attract bugs, no matter what. Always. So I always tell people, I kinda joke and say, let’s say that you have a major gallbladder attack, the doctor says you need your gallbladder out. So they take it out, they clean out the inside, they cover it with, you know, fill it with bleach, let it sit there a little while, and then they fill it up with some rubbery stuff and put it back in you. Why don’t they do that?
Jannine Krause (11:55.973)
Thank
Jannine Krause (12:15.663)
Dead tissue.
Michelle Jorgensen (12:16.782)
It’s a dead tissue and that dead tissue will attract bugs, right? Always. It will always reinfect. So the same thing happens in your tooth. You’ve entombed it now. Now the blood vessels aren’t there, so you can’t get immune cells into these areas anymore. There’s no flow. So the bugs find the dead stuff and now your body has to nonstop fight this low grade chronic infection.
Now, some bodies are fine with it, right? They don’t have any other things impacting them and impacting the immune system, distracting them, all those things. So it can keep it at bay. It can keep the infection from spreading. It’s just real localized, not a big deal. But what is it doing to the immune system as a result? I like it. It’s just distracting. Like it has so much to do all the time that something else comes along and it can’t deal with it.
And this is the connection between root canals and autoimmune disease because all of a sudden the body is so distracted over here, it can’t deal with other things. It just starts to like shoot at everything and that’s autoimmune disease. like taking you taken out its own cells because it doesn’t know what to fight anymore. It’s so distracted and tired. Even things like cancer. Cancer is just simply a cell that’s gone awry. Usually the immune system kills it. Well, if your immune system is distracted doing something else nonstop 24 seven, it may not be as capable of taking care of that.
So there’s so many diseases that relate and I will never say that the root canal caused cancer. there’s no way we will not ever say that, but the root canal leads to immune system function decrease. your immune system is not as good as it used to be, which then leads to the other disease processes taking hold and the body not being able to take care of them as well. So this is why it’s so important to identify what is the status of this root canal.
Is it still fine? Is the body taking care of it okay? And sometimes even people will say, I don’t even care because I don’t want my immune system to be compromised and not capable of taking care of me for other things. You know, just, just get it out regardless. But this is so fascinating. The way we find these is on what you’ve already mentioned. It’s called a cone beam CT scan. So what is that? It’s a special CT scan that a dentist can do. Now the machine looks a lot like something that we probably have all had. called a panorax where it goes around your head. Don’t mistake the two.
Michelle Jorgensen (14:28.418)
They’re not the same thing. A panorax is a two dimensional image. I can look at it on a screen, but I can’t tell anything depth wise. can’t go cut by cut by cut. I can’t look at anything that way. I can’t look at the bone. I can only see certain amount of things on that. This is a three dimensional image. I can literally turn your head inside and out. I can cut it slice by slice. I can see exactly what’s going on everywhere. So one of my favorite stories is really the time that my mind got changed on this.
I had a patient that came and she had a root canal on it. I always remember it was an upper, upper bicuspid. So an upper tooth like right in the middle here. And she just tapped on it. She said, I don’t know, every, every since I had this root canal just, just feels off. And that is the most common thing people say. It doesn’t hurt. It doesn’t really bother you. Remember the nerves gone, you know, but she’s like, I don’t know. just, I just feel a little off. So I took a regular dental X-ray, the kind that goes in the mouth. You know, you put it in the mouth is snap it and you look at it on the screen and took a regular dental X-ray. said, it looks just fine.
If any dentist had looked at that root canal, they would have said, it looks just fine because it did. But I had just gotten my new cone beam CT machine. So I said, you know what? Let’s go take a scan. I’m just super curious. Like, I don’t know. I think it’s going to be fine, but let’s just go look because it feels off. You know, let’s go look. We took a scan and my jaw dropped. There was a quarter size hole eaten in her jawbone all the way through from the tooth all the way out to the cheek side. Quarter size hole with bacteria eating away the jawbone.
I couldn’t see it on the dental x-ray. Could not see it. And this is what we find every single day. We can’t see them on regular x-rays. So it’s not that dentists are ignoring it. They can’t see it. They cannot see it. You have to get the cone beam CT scan. So when you’re calling a dental office, you say, do you have a cone beam CT machine in your office? Or do you have someone that I can go to to take it and bring to you at my appointment?
Jannine Krause (16:04.549)
Great.
Michelle Jorgensen (16:22.54)
because you must have that scan to be able to determine what is the status of these root canal teeth. If you’ve had a root canal at all, but not just that. mean, I find dead teeth in people’s mouths that have never hurt, that are completely infecting their sinus. Like someone will come in, they’ll have chronic sinus infection, have gone through three sinus surgeries. The ENT can’t figure out why it keeps filling back up again. We take a scan and I say, it’s because your upper molar is dead. I didn’t, I don’t know. I’ve never had root canal on that. It’s never hurt. I know.
But for some reason when you had that crown on the tooth, it killed the tooth, didn’t hurt. Tooth dead has eaten its way through the floor of the sinus and it’s unloading or basically draining all the infection into the sinus. So the ENT comes in, cleans it all out. Everything’s good to go for about three weeks. And then it fills right back up again because that tooth has to drain somewhere. So we find this day in and day out. That’s why in my practice, you never have an exam without a cone beam CT scan because there’s so many things we find.
So that’s the root canals. I’m going to jump to the other infection real quick just so we can finalize this answer, this story here. So the other places where teeth are removed and a lot of times people will say, well, I’ve never had a tooth removed. Wisdom teeth. yeah. I had my wisdom teeth removed. I was like 15. Exactly. So here’s the problem. So when a tooth is removed, there’s something called the periodontal ligament around every tooth. It’s just the way the tooth works. It’s why we can, when we bite on it, gives a little give to it. I think of it like a trampoline and like the springs, you know.
So this ligament surrounds the tooth and kind of holds it in this little basket. Well, when the tooth’s removed, the ligament doesn’t come automatically with the tooth. It has to intentionally be removed out of the area as well. When it’s not removed, what happens is the body doesn’t actually know the tooth’s gone for about 10 days because the ligament is the feeder. It’s what all the nutrients come to that tooth through from the outside. So the body thinks the tooth’s still there until that finally the ligament necrosis, it’s dead and the body goes, there’s a tooth gone.
But in that 10 days time, the gum grows down into the hole, but the bone doesn’t initiate healing because the body doesn’t think it’s too scone yet. So it thinks that there’s a hole in the gum. yeah, something happened here. Let’s go heal the gum. The gum grows down in. So you end up with this dead ligament basically entombed now in the jawbone. So the gum grows over top. It doesn’t really grow bone in here. Well, that dead ligament creates an inflammatory situation. So a lot of inflammation that we find in bodies and people who have had, you know, tests where
Michelle Jorgensen (18:47.832)
testing CRP, we’re testing all these inflammatory markers and people are, their doctors are like, I don’t know where this is coming from. Why are your inflammatory markers higher? We’ve dealt with everything we can think of. Have you checked the wisdom teeth areas? Because these will initiate a huge inflammatory reaction. And this is the really interesting thing. In the mouth, every single tooth is connected to organ systems. So this is, this goes along with Chinese traditional medicine. Every single organ system is represented on the hands.
Jannine Krause (19:01.893)
No.
Michelle Jorgensen (19:17.482)
on the feet, on the ears, and on the teeth. Isn’t that interesting? But I liken it to, it’s the charging system for every organ. So think about how much use we get with our feet, how much use we get with our hands, even our ears. You know, we get a lot of wind, you know, and things going on and our teeth. How many times do we put our teeth together? Every single time we swallow, every single time we chew. So I believe this is the way the body recharges itself. Every single time you chew, it recharges a little bit into the organ systems.
So the organ system connected to the wisdom teeth is the endocrine system. This is all the hormones. This is particularly sex hormones, estrogen, progesterone, testosterone. This is your get up and go, your thyroid, your adrenals. So, so many times people are just dragging, like, why do I feel so lousy? I’ve done all the hormone things. I’ve done hormone replacement. I’ve done all of this. Why do I still feel so tired, so rundown?
We go check these, we find, okay, four areas or three areas or whatever it is didn’t heal right after wisdom teeth were removed. And we’re looking for bone density. I’m looking for a hole in the jawbone basically. If that’s there, we go back in, we open into that hole, we clean out that dead ligament, we disinfect it to make sure there’s no bugs living in there. And then we fill it up with stem cells. So it will finally heal. And one of my very favorite stories of this is a lady, she literally had to move home with her mom. was in her early thirties.
She’d been, she’d worked in tech, but she was like travel was her love. So she had all these dreams to go travel the world. She actually had to move home with her mom because she was nearly bed bound. She could not figure out what was going on. Took a look on the comb beam CT scan, found four areas where her wisdom teeth hadn’t healed. And she had an infected root canal right here on her front tooth. She’d hit this tooth when she was like 10 on a bike and it had had a root canal. We took the root canal out. We cleaned out all four wisdom teeth areas. The next morning, her mom woke up and she heard something in the kitchen. She was like, what is that over there?
Went and looked, her daughter was up doing dishes. She was like, what are you doing? She said, I feel better than I felt in a decade. The day after getting this infection, this inflammatory basically thing that’s leading the body to say, fight me out. All of a sudden, the body goes, thank you very much. Now I can go on with the rest of the business that I want to do. So this is why you have to have a comb beam CT scan. We actually cannot see areas where teeth were removed on a regular X-ray. We can’t tell. We have to use a special
Michelle Jorgensen (21:43.318)
value indicator that tells us bone density and it can only be done on a cone beam CT scan. So you’ve got to have that scan to get a true exam to be able to look for root canals or areas where teeth were removed that didn’t heal right.
Jannine Krause (21:56.537)
my goodness. So valuable, so valuable because when I look at thermography, we’ll see that folks have inflammation in their jaw. We’ll see it kind of draining down the lymph. And then I see it go towards the breast and I start thinking about breast cancer. My mom and my aunt both died of breast cancer. And it’s one thing I’m like, I really need to think about this. And I think a lot of people might be thinking, could there be something there in that connection too?
Michelle Jorgensen (22:02.839)
and
Michelle Jorgensen (22:07.84)
Yep. Yep. Yep.
Michelle Jorgensen (22:21.986)
Yep. I have not found a patient yet that had either had or has cancer that doesn’t have an infected tooth. Haven’t found one yet. And nearly 100 % of the time when someone has breast cancer, I say, which side was it on? It was in the left side. I find a root canal on the bicuspid. So it’s not the, it’s not the eye tooth or the cuspids, it’s ones right behind it. I find a root canal either top bottom on that same side, because that is the meridian or the energy connection with the breast. So when you have a short circuit here,
Jannine Krause (22:31.757)
Huge.
Michelle Jorgensen (22:51.19)
infection here, it will lead to your body’s inability to take care of the breast or anything else on that same circuit. Huge.
Jannine Krause (23:00.567)
And so if someone’s feeling like sensitivity right now, maybe they have another root canal, but they’re feeling sensitivity in any of those areas, that would be like, go get it checked out right away. Let’s get a cone beam. Let’s make sure we can get on top of this.
Michelle Jorgensen (23:13.582)
Yep. And really interesting. One of the other teeth that was commonly removed, especially you told me your demographics like 35 to 55, you know, especially in that 55 here, um, generation is taking teeth out for braces. We don’t do this. At least we try not to do this anymore. creates so many issues. I call it the ambient generation because we’ve now made mouths so small that tongues can’t fit and all of a sudden nobody can breathe at night. So they’re awake all night. Nobody can sleep. They’re all on ambient.
Anyway, that’s a whole nother talk, but when those teeth are removed, the teeth that are removed are bicuspids. So if you’ve had breast cancer, you had teeth out for braces, you may have an area that didn’t heal right after those teeth were removed when the brace, when they were taken out for braces. Also a very common connection.
Jannine Krause (23:59.973)
I never even thought about that. That, I mean, that’s huge. That’s huge. I do want to get into the airway and the sleep evaluation that you do because I think it’s, you know, so many people are trying to avoid CPAPs because that seems to be like, all right, we end up being Darth Vader. And I don’t think that is really the answer either in this case. I mean, having a mask on yourself and a whole tube thing, like how, how was that even? I mean, to me in my mind, I’m like, that doesn’t even sound right. So.
Michelle Jorgensen (24:02.838)
Yep. Yep.
Michelle Jorgensen (24:16.11)
Well, it’s not as good as me.
Jannine Krause (24:28.005)
I would love to get your opinion there, but really quick before we move there, because I have something in my head that I wanna just get out, with the little tubules that are in the teeth. A lot of people talk about the different types of toothpaste, like the, I’m gonna probably say it wrong, hydroxyapatite, am I saying it wrong? Is that what those are doing? Are they putting, is that how that works? Just curiosity.
Michelle Jorgensen (24:43.04)
Yep.
Michelle Jorgensen (24:48.852)
Let’s this is a great question. I think it’s really important. So can we do the fluoride fluoride talk along with this? Okay, alright, so the idea of fluoride is awesome. It actually does strengthen a tooth and this was found in the 1940s. They would look at people who had lower cavity levels and they found that often they had higher fluoride levels naturally in their water. They were using well water and so they had higher fluoride levels and they said this is awesome. We’ve figured out how.
Jannine Krause (24:54.905)
Yeah, let’s do it. Let’s do it.
Michelle Jorgensen (25:17.004)
to completely get rid of cavities. So what fluoride does is it just strengthens the crystal that teeth are made of. So teeth are made of a mineral complex called hydroxyapatite. The exact word you just said. That’s what teeth are made of. So when you smile, you’re looking at hydroxyapatite crystals. What fluoride does is it incorporates into the hydroxyapatite, pushes calcium out and fluoride moves in. It creates something called fluorapatite. It’s harder, so it’s more resistant to acid dissolving it and it’s more brittle.
which is fine if it’s a tooth. But here, because tooth teeth have kind of a squishy layer underneath, okay? So it’s fine to have that brittleness because it has a little bit of give in that tooth itself. But here’s the problem. Anything you put in your body, and I’m sure you talk about this, anything you put in your body acts on the cell you want it to act on, but it also acts on every other cell in the body. And we call this in the medical world a side effect.
Jannine Krause (26:13.327)
Mm-hmm.
Michelle Jorgensen (26:13.71)
Well, a side effect is just simply the way that biochemistry works. No matter what we put in our body, it’s going to act on every single cell. Some things we want it to do, some things we really wish it didn’t do, but we don’t have a choice. It’s going to do it regardless. Fluoride has the same thing. It’s going to act on every single cell. So in a tooth, it’s great. It makes your tooth stronger. But the other thing that’s made of hydroxyapatite is bones. Same crystal. So now fluoride also pushes calcium out of the bone and incorporates and creates fluorapatite, which is stronger and more brittle.
Does anyone have a worry about a brittle bone?
Yes, so density increases, density changes in the bone itself and now we have higher rates of fracture in areas that are highly fluoridated. So okay, so now we have a side effect that we didn’t want, but I do want to establish one thing right at the beginning. Fluoride, the goal was to eradicate tooth decay. So did it do it? Has anyone had a cavity since 1940?
Jannine Krause (27:09.221)
Yup.
Michelle Jorgensen (27:10.382)
Okay, so we can establish that it did not achieve its goal, correct? All right, did it slow down to decay? Perhaps. Lots of research shows that it slowed it down. It didn’t stop it. Okay, so it didn’t stop it. It now creates brittle bones. It didn’t stop there. It also affects other things. So fluoride is very similar to iodine. If you look on the periodic table, they’re cousins. Fluoride, iodine, chlorine, bromine, they’re all what are called halides. But fluoride is the biggest cousin of them all.
Jannine Krause (27:13.989)
Yeah. Right.
Michelle Jorgensen (27:40.695)
So if it’s in the same area, it will bully iodine and push it out. So you know, I’m sure that thyroid hormone is activated by iodine as is the the cells that secrete stomach acid are also activated by iodine. Most cells that secrete something are activated by iodine. Well, if we have fluoride in the system, fluoride pushes iodine out. So now you do you do a blood test and you test thyroid hormone and it comes back as completely normal. But what it is is it’s thyroid hormone activated by fluoride.
not by iodine, and it’s not usable by the body. So in the 1970s, fluoride was used as a treatment for hyperthyroidism. They knew it decreased thyroid function. It was actually intentionally used as a medication when someone had overactive thyroid function. They used it intentionally because they know it does. Well, how many people do you know that have thyroid issues?
Jannine Krause (28:34.007)
Lots of them. Mm-hmm. Lots of them.
Michelle Jorgensen (28:35.138)
Yep. And how many people are exposed to fluoride through their water, through their toothpaste, through their mouthwash, through whatever it is at the dentist’s office? So much fluoride exposure. So fluoride simply counteracts the effect of iodine. So second, second strike against it. Third strike against it came actually early this year, 2025, January, there was a study published that showed that mothers that had higher levels of fluoride in their system led to babies that have lower IQ.
And they equated it one to one higher. This goes the lower. goes protector, particularly in male children. So it’s affecting the brain function as well. So now we’ve got bones, thyroid or energy systems and brain decrease in function and all of the three. So I say, okay, we were hoping to eradicate tooth decay. It didn’t work. It created all these other side effects. Was it worth it? Or maybe yours. It was, but not anymore because
Jannine Krause (29:28.549)
Bye.
Michelle Jorgensen (29:32.751)
cavities are not a deficiency of fluoride. They’re not. Remember fluoride wasn’t in the tooth to begin with. Hydroxyapatite, this mineral complex, is what’s in the tooth. So when you get acid on the tooth, either because you eat sugar and the bacteria in your mouth eat that sugar and then they create acid, so it’s not the sugar that creates the cavity, it’s the bacteria eating the sugar. So you eat a lot of sugar, bacteria stay on your teeth in plaque and then they eat it, they create acid. Or you drink acid or eat acid. Energy drinks.
You know, of these things, soda, even lemon water used all day long as acidic. And what it does is it just dissolves the minerals out of the tooth. So now it leaves a porous tooth behind. Well, if the tooth is porous, has holes in it, bacteria crawl in. Now it’s harder to clean them because there’s bacteria deeper in the tooth. They eat more sugar, they create more acid, they make a hole deeper. So this is what cavities are from, is simply acid dissolving hydroxyapatite.
So we used to fix it with fluoride. Well, let’s just make the crystal stronger so it doesn’t dissolve as easy. But now I’m saying we don’t have to do that because a cavity forms when hydroxyapatite is lost. Let’s just put hydroxyapatite back. That’s all we’re doing. So yes, going on the tubule idea, this enamel crystal idea, this porosity of the tooth, let’s just fill up all those holes with the mineral that a tooth is made of anyway. Let’s put back what was lost. And now we’re healing cavities.
We’re preventing tooth decay. Research shows that it is just or even more effective than fluoride was at preventing tooth decay. There is no need for fluoride in our world ever again. Period.
Jannine Krause (31:09.497)
Good deal, good deal. I hope that someone who I’ve seen before for dentistry hears this. And for the waiver I had to sign for denying that I did not want fluoride. Because I was like, really, I have to a waiver?
Michelle Jorgensen (31:21.26)
Yeah. And you know, I’ll talk to dentists about this all the time because we were, this was our doctrine. Okay. We were taught that fluoride saves teeth and that it’s really malpractice to not offer fluorine. This was, this is our doctrine as a dentist. I was just on two huge dental podcasts just last week and I, and they said, boy, you are killing some sacred cows here. I said, I am, but it’s okay. It’s okay to say we didn’t know. And we were doing our best.
and we were doing what we thought was the very best thing and perhaps for years it was. But now we have a better choice. And it’s okay to say that. mean, how many things in medicine have changed? Are we treating pneumonia the same way today as we were treating in 1940? Absolutely not. So why do we have to stand so resolutely on fluoride? We don’t have to treat it the same way today as we were in 1940. It’s okay. And that’s what I’m trying to tell the dental profession. It’s okay to say we didn’t know. And hey,
Great news, we have something even better now. We have hydroxyapatite now. So yeah, I actually started a product line myself because of this. Because I was like, we’ve got to have hydroxyapatite products that are good. That we don’t have other things that they add in that we don’t really want or need. So we have, know, toothpaste, toothpaste, mints, mouthwash, because there’s no need for fluoride. You just use hydroxyapatite.
Jannine Krause (32:44.461)
Amen. Amen on that one. my goodness. I’m glad you went through that. Cause yeah, it’s, it’s, it’s shocking, but I get it. You know, we, don’t know. And that, you know, I’ve amended lots of different things as even as a naturopath, different things, we just didn’t know. And here we are. And same thing goes, I think with the airway and sleep, if we go back to that, because I think right now, I mean, yes, it’s becoming a little more aware that there are dental appliances, which I don’t know. We’re to talk about that. I definitely want to talk about that because I’ve had a couple people have some
Michelle Jorgensen (32:52.91)
no.
Michelle Jorgensen (33:11.074)
We’re talk about it. Yep.
Jannine Krause (33:12.345)
some issues on that and then we have the night lace, which is the surgery. And then we have of course the CPAP, which everybody’s like, my gosh, Darth Vader, that can’t seem right. So what are you guys doing to move the needle a little bit forward in that department?
Michelle Jorgensen (33:28.44)
So first thing we’re going to do is we’re going look at the cone beam CT scan. I might sound like a broken record right now. And you have to have a cone beam CT scan large enough to see the airway. So this is also something to ask because there are cone beam CT machines. It’s called field of view. So it’s the size of the scan they’re going to take. Some take it just right here. They take just the teeth. They don’t even go back to the jaws, the jaw joints itself. And they certainly are not going to go back to the airway. So you need to ask for a cone beam CT scan that’ll show the airway.
Jannine Krause (33:34.211)
Okay.
Michelle Jorgensen (33:58.317)
So it has to be a large enough field of view, that makes sense to people, know, a large enough scan that we’re gonna see all of this. So we look at it and we say, what is the structural issue? Is there a structural issue here? So I’ll tell you, there’s two kinds of sleep apnea. There’s one called central sleep apnea, which is where your brain doesn’t tell your body to breathe. It is incredibly small percentage of apneas are actually central.
Jannine Krause (34:05.53)
I’m sorry.
Michelle Jorgensen (34:24.994)
The large majority of apneas, like I’m talking like 98 % of them are what’s called obstructive apnea, which means there’s just something in the way of air passing. So let’s talk about this. There’s a tube that goes from your nose past your mouth and down to your lungs. Okay? So it starts in your nose, goes all the way down, passes back behind you when you say, you’re looking at it, right? You’re looking at the airway, what we call the airway. So obstructive apnea means something is pushing its way back
into that tube and not allowing air to pass. So let’s talk about the fallacy of a CPAP right now. The CPAP doesn’t fix anything. What they’re doing is they’re just forcing more air into a pipe. So let’s say that you have a blocked pipe on your kitchen sink, right? Nothing’s going down, your sinks backing up. So does it work just to put more water through that?
No, now your sink just backs up even more. And a lot of people with CPAPs tell me that’s the problem. Literally the mask gets blown off their face and they get air in their eyes and their eyes are dry all night long. And why? Because you’re just trying to push more air past a blocked pipe. Does that make sense? So really there’s a huge fallacy with this. The other thing that’s a problem is when you force that air in, you’re now turning off your body’s own reflex to take a breath.
Jannine Krause (35:38.821)
Thank
Michelle Jorgensen (35:49.549)
So you’re actually making the problem worse. You’re kind of driving into central apnea or don’t breathe because you don’t have to anymore. I’m providing you the oxygen you need. So now you’re turning off the body’s own response to actually breathe more. And you’re just forcing it past a clogged pipe. It doesn’t work. So we have to stop and say, well, why is the pipe clogged? Let’s figure this out. And are there things we can do about it? So the largest thing, the largest problem we see is when mouths are too small.
When mouths are too small, if you think about the mouth, it’s like a closed box, right? You put your teeth together, everything inside of the teeth has to fit. Well, if the mouth is too small because they took teeth out for braces or because they didn’t do an expander, you have crooked teeth, you know, everything’s kind of crowded in there. There’s just not enough space. Well, now there’s not enough space inside of that box for your tongue, for the tissue at the back of the throat, for the tonsils, for any of that to fit where it should fit. So what does it have to do? It doesn’t have a choice. It has to spill backward.
back into the tube. So I liken it to like a big, long pickup truck that you’re trying to fit in a tiny little garage. No matter how far you try to shove that pickup truck in the garage, it’s gonna spill over onto the driveway no matter what because it’s too small of a garage. So we’ve got to make the garage bigger. Does that make sense? We just have to make the garage bigger. So we use expansion appliances that actually make the mouth bigger. We can do this in adults. We love to do it in kids.
Jannine Krause (37:08.268)
Mm-hmm. Mm-hmm.
Michelle Jorgensen (37:16.652)
So we love to find kiddos that are struggling with airway. And how does this show up in a kid snoring, mouth breathing? You hold your mouth open at night because that brings the tongue forward, brings the tongue forward and down. And all of a the air can get by. So as an adult too, if you’re mouth breathing, this is a sign you have a clogged pipe. You can’t get the air past kiddos the same. If you’re snoring, if you’re mouth breathing, if you’re tossing and turning, if they’re bedwetting, if they don’t have focus during the day, these are all signs they’re not getting air at night. So what do we do in a kiddo? Awesome. Let’s make the mouth bigger.
And an adult, what do we do? Let’s make the mouth bigger. So we have ways, we have appliances to make the mouth bigger. And this is the only appliance we use. Why? So the appliances you’re probably familiar with are the ones that bring your jaw forward. The concept is good because when you bring the jaw forward, it brings the tongue with it. So remember, we’re unblocking the pipe. This is great. But the problem is, that when you bring the jaw forward and hold it there all night long, the jaw joint itself is held in place. There’s a little piece of cartilage in that joint that’s held in place with a ligament.
Jannine Krause (38:03.717)
Thank
Michelle Jorgensen (38:15.894)
and the jaw itself is moved forward and back with muscles. When you move that jaw forward and hold it in that fixed position all night long, you overstretch the ligaments of this entire joint structure. It’s just like with a knee. You get ligament laxity. Now all of a sudden, the cartilage that sits in that joint doesn’t stay on top of the joint anymore. You get popping and clicking. Eventually, it just kind of falls out of that joint, and now you have bone on bone, which is arthritis. This is an acquired arthritis situation.
Jannine Krause (38:42.755)
you
Michelle Jorgensen (38:43.628)
Research shows that four years into using these appliances that hold you in a fixed position all night long, four years in, you’re gonna have irreparable joint changes. So we do not do these appliances because they aren’t fixing anything again. They’re just band-aids. They’re just holding it forward, but they’re not fixing the real issue, which is that there’s not enough room in the mouth for the tongue and the tissue. So we make space in the mouth. Now you said nightlays. What is that?
Well, sometimes the tissue at the back of the throat gets so stretched out because it’s been stuck in this airway, in this flow of air, and it gets stretchy. So night laser actually isn’t a surgery. So I’m so glad you said that so we can talk about what it is. It’s a laser light that shrinks tissue. It stimulates collagen formation. So we’re not cutting anything off and you don’t even get numb for it. All it’s doing is it’s stimulating the collagen fibers in the roof of the mouth and it’s causing them to shrink up. So we’re just shrinking the tissue up and out of the way.
Now it’s not a forever thing. Usually we do about three or four times and then we have to do a touch up about every year, but we may need to do it even along with the expansion. So we make the mouth bigger, but this tissue, it’s like if you lost 50 pounds, you still have the flabby skin. You know what I mean? Even though the 10 are gone, you still have the flabby skin. We got to shrink it up and get it out of the way. So we may need to still shrink the tissue. Infection in your mouth can lead to that tissue getting swollen. So the first thing I look at if you have airway issues is do you have an infected tooth?
Jannine Krause (39:53.699)
Okay.
Michelle Jorgensen (40:07.97)
or an area where tooth was removed that didn’t heal right because it can lead to all that tissue getting swollen and now getting pushed back into the airway. So does this make sense? We’re not just going to band-aid it and say, here, let’s shove some more air in your nose and through a blocked pipe, or let’s just like shrink up some tissue. We’re going to say, why is the pipe blocked? Is there an infection that’s leading to swelling? Is the mouth too small and why are mouths too small? Why do all of us have to get our wisdom teeth out? Why is everyone getting braces these days? Because of nutrition.
Jannine Krause (40:26.181)
Yeah.
Michelle Jorgensen (40:37.336)
first bone that’s affected by malnutrition. And I’m not talking like we’re starving, you know, I’m talking that the food we eat doesn’t have nutrients anymore. The first bone affected by it is the top jaw. So I learned this because of my son. I adopted him at two and a half and his top jaw was so small. It was literally completely inside of his bottom jaw because he was so malnourished. And I was like, why is his jaw like this? And I did a bunch of research and found out it’s the first bone affected by malnutrition.
So when you have malnutrition, you’re just not getting enough nutrients. The top jaw forms narrow. The bottom jaw then has to form narrow. And now we know everybody ends up with braces. Everybody ends up with no room for their wisdom teeth. This goes back to nutrition. So everything I do is hitting nutrients, vitamins and minerals, vitamin D3, K2, starting at an infant. And all of you adults who need to do this as well. And then minerals that can strengthen teeth, but also help.
to grow bones, help your bones to be what they need to be and wide enough. So when you have sleeping issues, the first question is why? Why? What’s blocking? Is this my brain not telling me to sleep 2 % of the time or is this something blocking my airway 90 % of the time? What’s blocking it? Why and what can I do to fix it?
Jannine Krause (41:39.749)
to make sense.
Jannine Krause (41:53.701)
makes sense. That makes sense. You have heard a lot of stories of the different appliances, obviously the CPAP machines and and nightly. Yeah, that’s kind of newer. And so obviously, I’m still trying to figure out what that is. So that makes sense. Now, on the side of, know, GLP ones are very popular right now. A lot of people are using it for losing weights and some people are using it to basically get super thin.
Do you have any thoughts on what might happen with the teeth on that side of things? Have you seen anything? What’s going on there?
Michelle Jorgensen (42:25.964)
Yep, so this is being dubbed like GLP one teeth. So the problem is, in fact, fascinating story. Literally just last weekend, I was at a wedding and I was close friends with the bride’s family. So the other side of the family, her mother found out that I was a dentist and we were in the kitchen cooking and we were prepping for the wedding and she said,
She’s like, I have had the biggest issue. She’s like, I’ve never had cavities in the past. And all of a sudden, all I do is get cavities all the time. And my dentist cannot figure out why they put me on all this fluoride and everything else. And I said, okay. So first of all, it’s either you’re not taking care of your teeth, right? But that sounds like that hasn’t changed. So that’s usually what everybody’s blaming cavities on. The second thing is, is you’re not absorbing nutrients properly. And she looked at me, she said, I had a gastric bypass. I said, bingo.
So here’s what people don’t understand. The same thing is gonna go with gastric bypass as GLP-1s, all of these things. What it’s doing is it’s affecting the absorption of nutrients in your gut. And when that happens, your body needs a certain level of minerals to operate. Your brain needs minerals, your heart needs minerals. If your body is not getting enough because your absorption rates have changed, which is this, this is what happens. You get a lot of
poor motility. know, sometimes stomachs even stop working entirely when you’re on GLP-1 medications. So now you’re not absorbing minerals properly. Well, when you’re not getting enough to run your heart and your brain, your body has to go mine them from somewhere. Guess what two ready-made banks of minerals are? Teeth and bones. So now we’re seeing people on these medications with rapid tooth decay and osteoporosis.
because their body has to get the minerals for somewhere, the brain and the heart stops and the brain and the heart take precedence over your teeth and your bones. Because you can live without teeth and you can live with weak bones, but you can’t live without your brain and your heart. So this is so huge. If people feel like, gosh, I’ve changed nothing, but why am I getting cavities? Especially along the gum line. If you’re getting cavities along the gum line, this is nutrient deficiency all the way. So what do you do about it? Well, I like to do something called the baking soda test.
Michelle Jorgensen (44:46.114)
This is my favorite little test. Maybe you’ve done this. So you take a quarter teaspoon of baking soda and a half a cup of water, mix it up and drink it. What are you doing? The baking soda should be reacting with stomach acid. So we like to this first thing in the morning before you’ve eaten any food should be reacting with a stomach acid. You should burp in two to three minutes because that reaction, it’s like when you know, your kid does that science fair experiment with the day, dump baking soda and the vinegar in a volcano, right?
The baking soda interacts with the stomach acid and it creates a chemical reaction. It creates gas. So you should burp in two to three minutes after drinking this. Quarter teaspoon of baking soda, half cup water. If you don’t burp, what it means is you don’t have enough stomach acid to actually break your food down, including minerals. Minerals have to be ionized by stomach acid. So if you’re not burping, automatically I can tell you, you are not absorbing enough minerals to keep your body healthy. This is why you’re getting cavities. This is why you’re getting osteoporosis. This is why you’re getting these other issues.
So the first thing we deal with is stomach activity. And I know a lot of GLP-1 people have to deal with stomach activity. In fact, I have a new formula just coming out that’s called stomach reset for particularly these people because it resets the activity. We’re using a lot of old Indian, Ayurvedic herbs and things to try to reset the stomach motility, get stomach acid working, but you may need to supplement stomach acid right now. You just got to take it. So you have to take something called betaine.
along with your food so that your food can actually be ionized, the proteins can be broken down so that they’re absorbable and recognizable so that you can use your food. You may just have to add betaine with your food for a little while right now. On the other end, you need a supplement with minerals. So I have something called tooth bone formulas, tooth and bone specific minerals, but also vitamins D3 and K2, because D3 grabs the minerals, K2 puts it in the cell. Otherwise you’re just gonna end up with kidney stones and gallstones and tartar on your teeth and things you don’t want.
You gotta have them in tandem, minerals plus vitamins together. So if you are on these medications and you’ve lost weight and all this, your stomachs aren’t working the same way as they used to be. So take the test, see if you need to add acid, but for sure you need to add minerals and vitamins.
Jannine Krause (46:53.957)
So, so important, so important. Thanks for taking that tangent for a second. Now you had mentioned that nutrition deficiencies in gums, we’re seeing cavities near the gums. Gum recession is a big deal. A lot of folks in my industry talk about it as related to gut health and tissue health. Some people talk about estradiol being affected there too.
What’s your take on gum recession as we get older and grafting doesn’t seem to be the solution is what I kind of saw on your website, but I want to hear your take in it. That’s just my impression there.
Michelle Jorgensen (47:29.784)
So there’s really two, three reasons that can lead to gum recession. Number one is gum disease. We talked about that at the beginning. If you have gum disease and there’s tartar underneath the gums, the gums will shrink away to get away from that tartar because the tartar is full of bacteria. The bacteria, I like to think of them as like bacterial condos. Bacteria are living in there, they’re dumping their garbage, they’re having parties. And like the gums are like, get me away. So they will recede. So if you have gum recession, the first thing you would check
is have your dentist, your dental hygienist measure your gum, say, do I have gum disease? I’m gonna tell you it’s maybe 30, 40 % of the people there’s a gum disease aspect. So what about everybody else? So the second thing that every dentist blames it on is you’re brushing your teeth too hard.
But this is the fallacy with this. Number one, usually it’s not every tooth. So if you look in your mouth, you’re gonna see, I have like recession, like right here on the side, you know, it’s the top and the bottom teeth, they’re touching each other right here and like right here. And man, those teeth are so sensitive. So then I say, well, why are you brushing those teeth so hard, especially if they’re sensitive? And they’re like, well, I don’t, I actually don’t brush those teeth hardly at all. Bingo. So it’s not tooth brushing that’s causing the problem. Why is it not every other tooth?
Why did you just pick that one to make the gum go away? So it’s not that. Sometimes it is in a very rare situation, but it’s not very common that it’s actually tooth brushing. So take that off your plate. It’s not your fault. The third thing that I find is the most common is the way the teeth fit together. Why are they right on top of each other, top and bottom? Because the way the teeth fit together. So if when the teeth hit, they should just be hitting pretty much straight up and down mountain into the valley. But if the teeth sit a little skew-ompous and now you’re getting mountain to mountain.
or valley to valley, or you hit on the mountain, then you slide down to the valley. What it does is it actually flexes the tooth. When the tooth flexes, the flex point is right at the gum line. So the flex point creates a little chipping right here, a little flexure, and the gum goes, I’m going to move out of that flex zone. It’s kind of like the splash zone at SeaWorld or whatever. I’m going to move out of the flex zone away from it so that it can keep flexing with this bite that’s a little off, and I’m not going to be affected by it.
Michelle Jorgensen (49:41.975)
I have now found a good solid part of the tooth to hook onto up here that’s not flexing. So this is why we see recession with teeth that are in contact with each other, because it’s the way they’re hitting together. So we go back and say, all right, is this an orthodontic issue? Do we need to move the teeth out of the way? Is this an expansion issue? Are you squeezing your teeth at night? Because when you squeeze, it tightens up all of the tongue and all the tissue in the back of the throat, and you’re able to breathe past it better.
So anybody that says, you know, I just not sleeping great. I clench and grind all night long. It’s because I’m so stressed out. I’m like, no, you clench or grind all night long because you can’t breathe. And your body knows as soon as it gets into deep sleep, your muscles relax. All that falls back into the pipe. It plugs it further. And your body says, no, you can’t actually be this relaxed. You have to squeeze your teeth together, tighten up your tissues so I can breathe again.
So now people aren’t sleeping at night because they literally can’t sleep and breathe at the same time. But what does it do in the meantime? All that clenching and grinding leads to gum recession because the gums move up and out of the way of the flex zone. So anytime I see just, you know, gum recession across the board, I’m like, you don’t sleep good, do you? People look at me like, how did you know that? Because the gum recession is because you’re trying to stay alive at night.
So we have to go backward. This is why we go back to the root of the root of the root. We have to figure out the main thing. So people can say, it’s gum, it’s gut issues that are your gum disease. And I can say, maybe, but most likely the fact that you aren’t sleeping has a lot to do with the fact that you have gum recession in every single tooth in your head. So sure, let’s fix your gut. That’s not always, that’s never a bad thing to do, but let’s actually get you breathing and sleeping without having to squeeze your teeth to do it. And then the gum recession stops.
Jannine Krause (51:32.985)
You bring up a really good point because a lot of women I’ve heard over the years do clench. It seems like it starts to happen as we get older. And so I can see how it’s easily said that, yes, there’s more stress, there’s more things we’re thinking about, the grinding kind of thing too, but it does make me wonder, like, okay, yeah, it would make sense if we’re gaining weight too at the same time.
Michelle Jorgensen (51:41.28)
You
Michelle Jorgensen (51:54.179)
You got it. Now all of a sudden your body. So think about it when you lay down, gravity is not in your favor, right? So when you’re in light sleep, your muscles are engaged. When you’re in deep sleep, less muscles are engaged. In REM sleep, it’s defined as paralysis. So you actually can’t engage a muscle. So when you drop into REM sleep, this is, I’ve heard it hypothesized. It’s so that we don’t like act out our dreams. You know, we don’t like run around and whatever. So when you were in REM sleep, your muscles have no tone.
So the tongue muscle, the back of the throat muscle, all of those muscles that have been holding the airway open to get enough air past now relax. So everything falls back. And if you can’t breathe past it, your body will not let you stay in that deep sleep mode. Immediately you will come out of it. So you’ll wake up and you’re like, why am I, why am I awake? You know, or you just, you know, toss and turn a little, as soon as you toss and turn, you’re out of deep sleep because remember that deepest level of sleep.
You’re paralyzed. You cannot toss and turn. If you’re tossing and turning, if you’re waking up, you are coming out of that deep sleep layer. So it’s just your body saying, I literally cannot stay alive and sleep deeply at the same time because I have added weight here because my muscle tone is getting older. Everything’s a little droopy, you know, whatever it is. I can’t do them at the same time. So you will not sleep deeply. You cannot do it anymore because you will not, you will not live if you do it. So you squeeze.
Jannine Krause (53:19.535)
Yeah.
Michelle Jorgensen (53:20.408)
Tighten everything up, now you’re not sleeping deeply, but at least you’re breathing.
Jannine Krause (53:25.219)
Nice. Well, I mean, it makes sense to kind of look in that and go, okay, all right, we’ve got other reasons than just working on the jaw. Yeah. Which leads us kind of to a little bit of root, but also I want to get into some of the advanced therapies that are common with holistic dentistry, in particular the ozone, the platelet-rich plasma, and those kind of treatments, because a lot of folks ask me,
Michelle Jorgensen (53:32.716)
at the root of the root of the root.
Jannine Krause (53:52.001)
about that and they’re like, do you think? Is it necessary? Do I always have to do that? Like, I think there’s a little bit of a thought process, at least in the Tacoma area, that we have, if we’re going to a biologic dentist or a holistic dentist, we are going to have to do the ozone or the PRP or something like that. Tell us a little bit about those particular procedures, how it ties in to improving oral health and how it can be beneficial based on certain conditions there.
Michelle Jorgensen (54:21.046)
So ozone is simply three molecules of oxygen. Oxygen likes to be an O2. That’s why we call it O2 all the time. Right. When you add a third molecule, it’s like that third wheel. It’s unstable. It doesn’t like a third to have a third wheel. So that unstable oxygen molecule will break off of that oxygen that that’s that triple quit. It will break it up. It will break off and it has to go and bind to something because oxygen likes to be in pairs. So now it’s got this free floating oxygen has to go bind to something. Well, the beautiful thing is
And when it binds to it, it does something called oxidizes it. And so we hear this word. So the reason when you cut an apple, it turns brown. That’s actually oxidized. It’s oxidizing when it’s exposed to the oxygen. So the same thing it does to the cells. It will oxidize something. Well, the beautiful thing is it loves to oxidize bugs, bacteria, viruses, fungus, parasites. doesn’t matter what it is. It will bind to it to stabilize the oxygen. But in the binding, it destabilizes the bug and kills it. It’s beautiful.
And then when the bug dies, its guts spill out and kill all the other bugs in the area. So it creates this chain reaction of killing, which is so amazing. So we use it in dentistry because we now are able to kill bugs without things like antibiotics.
So we’re able to use it topically. use it as a gas all the way around the gums. know, this is what we use to kill bugs in the mouth. We use it in a surgical site. Why? Because our instruments can only go so far. They can’t get into every little nook and cranny and make sure we’ve got everything. And I don’t want to use bleach anymore. So we use ozone. Why is ozone so amazing? Because the thing that it breaks down into is oxygen. Funny enough, we could use a little bit of that.
So we use ozone in this in surgical sites to kill bugs. We use ozone to desensitize teeth. We use it underneath deep cavities. Actually, we didn’t talk about this. People always will say, well, what do I do if I’ve been told I need a root canal? Well, what we do instead is instead of uncovering if the tooth is still alive, if the tooth is dead, your only options at this point are root canal or remove and replace it. We didn’t actually say what we should do about a root canal. If you’ve had a root canal, we remove the tooth and replace it with a ceramic dental implant.
Michelle Jorgensen (56:30.668)
But if the tooth is just a deep cavity still alive, what we do is we remove the cavity down to the deepest layer, but leave the nerve uncovered. That’s the key. We don’t want to uncover the nerve. We use ozone on that deepest layer of cavity to kill all the bugs. And then we fill over top of it. We have about a 92 % success rate of teeth that have been deemed, you need a root canal. We’re able to save them and keep them alive now, as long as they’re still alive. So we use it in underneath the cavity. So if I’m a patient,
I would not go to a biologic dentist that doesn’t have ozone. Because there’s so many ways it’s used that are beneficial. For gum disease treatment with antibiotics, for surgery to make sure that all the bugs are gone, underneath a filling to make sure that it’s never gonna turn into a root canal. So many different reasons. So that’s ozone. PRF, so PRP is platelet rich plasma. I used to use that years ago actually. I was one of the first users in dentistry of it. But now we use PRF, platelet rich fibrin.
because we want the fiber portion of it. It’s kind of a mesh because where we use it is where we want bone to grow. So we use it in sites where teeth have been removed. We use it in gum grafting areas. We use it where we want bone to grow because it gives a scaffolding that does a couple of things. It holds growth factor there for about 10 days instead of one day. The growth factor usually moves in and it moves out.
Jannine Krause (57:34.752)
you
Michelle Jorgensen (57:52.949)
It gives something that the bone can actually grow to. So we can say, we want it to be this high. We’re going to put the PRF this high so the bone will grow to it. It eliminates dry sockets because a dry socket is simply a socket that bone doesn’t grow in. Well, we put the PRF in now the bone grows there. So again, if I’m going to get an extraction done, a tooth removed, I’m not going to go to anywhere that doesn’t have PRF. But if you’re just fillings and cleanings, you don’t necessarily need someone that has PRF. Does that make sense?
It’s more in surgical applications that you’re going to use PRF. But for cleanings and fillings, I would not go to somebody that doesn’t have ozone because it is used in every single thing we do in dentistry. So hopefully that clears that up a little bit.
Jannine Krause (58:21.69)
Yeah.
Jannine Krause (58:35.343)
Would someone who normally has to take antibiotics before a dental procedure, could they avoid that if they made this on their own choice, of course, because I know standard of care is use antibiotics. Could you avoid that if ozone therapy was used saying that the person was signing off that that’s what they wanted to do instead of an antibiotic?
Michelle Jorgensen (58:55.628)
Yes, because we use the reason for the antibiotic is that bugs in the mouth, particularly particularly like hearts and joints. So if you’ve had a joint replacement or you’ve had a valve, you know, valve replacement in your heart, then typically it’s recommended for at least a year. The recommendations change, which is always funny to me. I’m like, well, parts and knees haven’t changed. Why are the recommendations changed? But they have. So I believe it’s now a year you should get pre appointment antibiotics. So
The idea is that if we’re stirring up bacteria and it’s getting into the bloodstream, they may go to your heart or your knee. So you may just choose for that year to do it, or you can use ozone. So in our office, we actually use ozonated water. So all of the water that we use. So any water that we’re spraying in your mouth, any water that’s coming out of the drill, it all has ozone in it. That is really important because you wanna make sure that anything that could potentially be getting into the bloodstream has ozone in it. So it’s gonna kill the bacteria that are potentially getting into the bloodstream.
So yes, ozone is very, very useful for that. One of the other things that people don’t think about, and it’s kind of disgusting, is that we dealt with this during the AIDS epidemic. One of the biggest chances for spreading of disease in a dental office is through our drills.
because they have water lines and the water comes back up in them as well. It goes out and it comes back up in. And so now if you have somebody who has something in their mouth, it can get back into the water line and any water line is a stagnant place that bacteria grow. And something called biofilms grow inside of the water lines themselves. They’re gross. It’s like why your water bottle’s like kind of slimy? That’s biofilm. So any sort of a water line will have biofilms in them.
So we, clear since the AIDS epidemic and dentistry have worked to make sure that we don’t have bugs growing in our water lines, but we’ve used all sorts of things like we used to use, everclear. We used to use Clorox. We used to use all these things that really aren’t so great for you, you know, now we use ozone because it kills every single thing in those water lines. So what this does is it eliminates the possibility of cross exposure as well. So I had a huge, huge, a whole bunch of dentists incorporate ozone in their offices during COVID because I said,
Michelle Jorgensen (01:01:06.112)
Your COVID risk of exposure and cross contamination is in your dental lines. It’s actually not the surfaces that somebody sneezed on. It’s getting sucked back up the dental line and then sprayed back out of the next patient. So ozone in those dental lines is absolutely imperative. It kills everything on contact. So we use ozone water in the lines, which is also gonna be beneficial in the mouth too and in the rest of the body too.
Jannine Krause (01:01:28.965)
I’m horrified not being a germaphobe. I’m like, my God.
Michelle Jorgensen (01:01:32.955)
So I know we’re short on time, but I’ve got to tell you this story because it’s so crazy. So we opened a new practice and we moved into another dentist’s practice. He’d been practicing there for 15 years. So I started working there at the time I was doing a lot of surgery and like full on, you know, eight hour surgery days. So it was one of my first days practicing in this facility and there’s a main vacuum trap on our dental vacuums and it’s like a big trap and it creates, it collects all the crap, all the disgustingness. I mean, it’s so gross. Okay. So it plugged up.
And I thought, that’s really interesting. He must just not have emptied it out. You know, he must’ve known he was selling the practice to us. He just didn’t empty it out. So we emptied it out. It proceeded to plug up 12 times that day. And I did not figure out what was going on until about two days later, two days later, I went, it’s because I’m using ozone water in the lines. It dislodged 15 years of bio sludge in that one day.
Jannine Krause (01:02:29.573)
God.
Michelle Jorgensen (01:02:31.646)
Is that not the most disgusting thing ever? So go to a dentist that uses ozone because everything is going to be clean squeaky clean. We’re actually just moving into a new office. It’s going to be our pediatric facility. And we said, we’ve got to remember this. We’ve got to run the water through the lines before we move in, because I guarantee we are going to dislodge because this practice has been over 20 years. We’re going to dislodge 20 years of crap in a day. We have to make sure we’re planning for this.
It’s just so crazy.
Jannine Krause (01:03:02.737)
Oh my gosh, I’m just so horrified right now that I’m like, oh my gosh, I don’t even I mean, because I’m thinking too about, know, we want to be thinking about water just in general, like what kind of water is being used, but then add the ozone and then oh my god, that’s Oh, okay. All right. I think you might have convinced a lot of people, including myself, that it is time to maybe ask more questions because I didn’t even think about I didn’t think about in the water and the lines now.
Michelle Jorgensen (01:03:13.858)
Yep, gotta have ozone. Gotta have ozone in that water.
Michelle Jorgensen (01:03:22.08)
Nobody does. Nobody does. Nope.
Jannine Krause (01:03:31.973)
So we probably need to do a whole podcast on all the other gross things. So I’m sure there’s other gross things that we didn’t even talk about today. But for the sake of time and just giving folks something they can think on besides being horrified, you know, for preventative dental care practices, know, obviously nutrition is important, things of that nature. you know, we’re always told like go get your dental cleanings and floss and brush your teeth. What other things would be
Michelle Jorgensen (01:03:37.539)
Exactly.
Michelle Jorgensen (01:03:43.854)
you
Jannine Krause (01:03:59.685)
crucially important that you like to tell folks to think about that they might not be thinking about compared to the usual recommendations. Okay.
Michelle Jorgensen (01:04:06.094)
So let’s just go through the list. You’re going to brush your teeth with a Hydroxyapatite Tooth Care product, either the tooth powder or toothpaste. Then you’re going to clean in between the teeth. I don’t care if you floss. You just need to clean in between them somewhere, somehow. My favorite is actually called a shower flosser. So it hooks between the shower head and the wall. And it’s like a water pick, but you’re already wet. It’s already in the shower. It’s already nice and warm, like it’s the best way, because
people that do water picks so I could make such a mess out of my kitchen, you on my countertop. I’m like, then do it in the shower. Spend one extra minute in the shower. It’s awesome. So just clean it between some way. Then tongue scraping. People often don’t know about tongue scraping, but a lot of yeasts live on the tongue. So you scrape the tongue and then you rinse. And I use a hydroxyapatite mouth rinse with colloidal silver. Colloidal silver is the antimicrobial and it makes a matrix with the hydroxyapatite, which holds it against the teeth. So now you have a, you know,
plaque or biofilm in your mouth that actually is reparative. It’s holding that hydroxyapatite against the tooth. It’s resisting decay so you get acid. It’s gonna take off that layer first and it won’t even touch your tooth. So hydroxyapatite mouthwash is the last thing I like to do. So that’s the scenario I recommend for everyone.
Jannine Krause (01:05:17.273)
Good stuff there, think that’s huge. It’s definitely things that I’ve started to incorporate over the last couple of years as well. And then last but not least, one of the biggest things that will happen is dental emergencies, like tooth chipping and things of that nature. What do you actually, well, first and foremost, if we have tooth chipping, we’re thinking about bone and bone density and things of that nature, but also.
Michelle Jorgensen (01:05:41.086)
and grinding and clenching.
Jannine Krause (01:05:43.91)
So seeing that as well. Okay. Okay. Got it. Got it. And so that’s what we want to be thinking about dental emergencies there, things of that nature. And I think, you know, I had something in my head and of course now I’m forgetting it, but I will probably come up with it later and I’ll just bug you later on it. But we got to tell everybody where we can find you, where are we your best found on Instagram. And then of course you have a book that we got that’s coming that we’ve got to have everybody talking about too. So.
Michelle Jorgensen (01:05:44.97)
Yep.
Michelle Jorgensen (01:06:10.914)
Yep, yep, so golivingwellwithdrmichelle.com. That’s the website. That’s where you can find product as well as all sorts of information. I’m just all about teaching people. So you can check us out on Instagram, Facebook, YouTube, YouTube videos. I release a YouTube video every single week. I just did one this week on root canals. And so there’s so much information if you want to know more, I guarantee you I’ve done a video about it.
So just check out livingwelldoktermichelle.com and the book is actually, it already did release in May and it’s called Living Well with Dr. Michelle. Also, the publisher insisted on that name, that it’s all about how to have unlimited energy, how to utilize your cells and work with them the way they already work and get that unlimited energy. So check it out. can learn about that on the site as well or livingwellbook.com is a place to go for that.
Jannine Krause (01:06:59.269)
Perfect, perfect. And then, you know, one of my things that I didn’t catch at the beginning of the podcast to let everybody know, I had you on my podcast way back in the day when I started episode 116, we were talking about, can you get…
Michelle Jorgensen (01:07:12.846)
Literally.
Jannine Krause (01:07:13.893)
from Root Canals and I didn’t hit it on it first and I sincerely apologize for not letting everybody know that like Michelle’s been on before but way back in the day back when I first started things and we were kind of already starting the conversation then but so many things have happened in dentistry and advances and I think this is you know great for folks to be thinking about that and you also have a resource in terms of if folks are not coming down to American Fork, Utah, where else they can go to try to find somebody that is doing similar work to you as well too.
Michelle Jorgensen (01:07:43.158)
Yep, on the website there is a dentist finder. So go on there and you can find somebody that’s close to home.
Jannine Krause (01:07:48.431)
Thank you, yes, my gosh. Thank you so much for coming back on and sharing so much great information with us. I learned a lot. I know folks are definitely gonna be learning a lot from this one too. And I think we’ll just keep a record of having you on every couple years so that we can keep the updates going. Because last time it really opened my eyes to a lot of stuff too. And now I’m like, okay, I gotta check a couple things like lines at the dentist’s office. I may be flying to Utah now.
Michelle Jorgensen (01:08:02.958)
Very
Michelle Jorgensen (01:08:09.391)
There you go. Thank you.
Jannine Krause (01:08:14.457)
Thanks again, Michelle, I really appreciate it.